Speaker Summaries (2023)
Monthly Meeting: December 6, 2023
Speaker: Dr. Sachin Kamath, Florida Cancer Specialists
Topic: Radiation Treatment
Thirty-four people attended our meeting on December 6. Nineteen people were in the audience and fifteen people joined on Zoom. Our speaker was Dr. Sachin Kamath, a radiation oncologist with twenty-five years’ experience. Dr. Kamath practices with Florida Cancer Specialists where he is a member of their Executive Board and Chief of Compliance. He also sits on the Board of Directors of the Florida Association of Clinical Oncologists.
Dr. Kamath stressed a multi-team team approach with a medical oncologist as the quarterback and urologists and radiation oncologists as cornerbacks. This differs from when he started practice when the urologist was the primary provider for prostate care patients (PCa).
If PCa has spread, it is not the end of the world. When he started practice, men diagnosed with Stage 4 PCa could anticipate a life expectancy of two to four years. Now they can look forward to fifteen to twenty years.
He advised patients not to be afraid of seeking second or even third opinions if a patient is not satisfied with the advice received from his medical provider. There are confusing options, many non-surgical, and patients must not feel pressured into choosing one he is not comfortable with.
Approximately half of the cases Dr. sees are more advanced where the disease has spread into the surrounding tissue but has not metastasized into the bloodstream or the bones.
Dr. talked about the radiopharmaceuticals Xofigo (radium 223) and Pluvitco (Lutetium 177).
Xofigo has been around for ten to twelve years and only attacks bone metastases. It will not treat soft tissue mets.
Pluvitco attaches onto a protein called PSMA that is found on the surface of PCa cells anywhere in the body in both hard and soft tissue. Upon binding, Pluvito destroys cancer cells by beta particle radiation. Pluvitco is not for everyone because not all men express the PSMA particle.
Regarding external beam radiation therapy, 10 years ago, 9 weeks of treatment targeting the entire pelvic area was standard practice. With current imaging capabilities, radiation therapy can pinpoint a much smaller target and increase dosage. In his current practice, 95% of his cases are hypofractionated with 5 weeks normally being the maximum treatment time frame and three to four weeks being common. As little as five treatments are also possible. He has found that the higher the dosage, the more effective the treatment.
Prostate size is not the deterrent that it once was. Most of Dr.'s cases range between 40 and 70 grams (1 gram of prostate weight approximates 1 cubic centimeter of volume). Prostates of 100 grams require procedures to shrink the gland normally with hormone therapy.
When tumors are located in multiple areas of the prostate, different dosage levels are utilized with the biggest tumors receiving the higher dosage.
Recurrent radiation therapy is possible with today's technology, particularly when lymph nodes are targeted.
Photon beams are X Ray beams while Proton beams are radioactive particles that kill cells faster and lose energy as they hit their targets.
Fred Barone
[email protected]
Speaker: Dr. Sachin Kamath, Florida Cancer Specialists
Topic: Radiation Treatment
Thirty-four people attended our meeting on December 6. Nineteen people were in the audience and fifteen people joined on Zoom. Our speaker was Dr. Sachin Kamath, a radiation oncologist with twenty-five years’ experience. Dr. Kamath practices with Florida Cancer Specialists where he is a member of their Executive Board and Chief of Compliance. He also sits on the Board of Directors of the Florida Association of Clinical Oncologists.
Dr. Kamath stressed a multi-team team approach with a medical oncologist as the quarterback and urologists and radiation oncologists as cornerbacks. This differs from when he started practice when the urologist was the primary provider for prostate care patients (PCa).
If PCa has spread, it is not the end of the world. When he started practice, men diagnosed with Stage 4 PCa could anticipate a life expectancy of two to four years. Now they can look forward to fifteen to twenty years.
He advised patients not to be afraid of seeking second or even third opinions if a patient is not satisfied with the advice received from his medical provider. There are confusing options, many non-surgical, and patients must not feel pressured into choosing one he is not comfortable with.
Approximately half of the cases Dr. sees are more advanced where the disease has spread into the surrounding tissue but has not metastasized into the bloodstream or the bones.
Dr. talked about the radiopharmaceuticals Xofigo (radium 223) and Pluvitco (Lutetium 177).
Xofigo has been around for ten to twelve years and only attacks bone metastases. It will not treat soft tissue mets.
Pluvitco attaches onto a protein called PSMA that is found on the surface of PCa cells anywhere in the body in both hard and soft tissue. Upon binding, Pluvito destroys cancer cells by beta particle radiation. Pluvitco is not for everyone because not all men express the PSMA particle.
Regarding external beam radiation therapy, 10 years ago, 9 weeks of treatment targeting the entire pelvic area was standard practice. With current imaging capabilities, radiation therapy can pinpoint a much smaller target and increase dosage. In his current practice, 95% of his cases are hypofractionated with 5 weeks normally being the maximum treatment time frame and three to four weeks being common. As little as five treatments are also possible. He has found that the higher the dosage, the more effective the treatment.
Prostate size is not the deterrent that it once was. Most of Dr.'s cases range between 40 and 70 grams (1 gram of prostate weight approximates 1 cubic centimeter of volume). Prostates of 100 grams require procedures to shrink the gland normally with hormone therapy.
When tumors are located in multiple areas of the prostate, different dosage levels are utilized with the biggest tumors receiving the higher dosage.
Recurrent radiation therapy is possible with today's technology, particularly when lymph nodes are targeted.
Photon beams are X Ray beams while Proton beams are radioactive particles that kill cells faster and lose energy as they hit their targets.
Fred Barone
[email protected]
Monthly Meeting: October 4th, 2023
Speaker: Dr. Lawrence Klotz
Topic: Is Focal Therapy Right For Your Prostate Cancer.
Our meeting was spent reviewing a video of Dr. Klotz's presentation. No summary is available but the video can be viewed.
View the video here.
Speaker: Dr. Lawrence Klotz
Topic: Is Focal Therapy Right For Your Prostate Cancer.
Our meeting was spent reviewing a video of Dr. Klotz's presentation. No summary is available but the video can be viewed.
View the video here.
Monthly Meeting: September 6, 2023
Speaker: Sara Sattler, Prostate Cancer Rehab Specialist
Topic: Urinary Incontinence
Our speaker at our hybrid meeting (20 people in the audience and 17 people on Zoom) on September 6 was Sara Sattler. Sara is a Prostate Cancer Rehab Specialist specializing in sexual and intimacy issues and urinary incontinence. She has a technical background in other medical specialties including organ tissue recovery. When her father and father-in-law were diagnosed with PCa, they turned to her for support, and she embarked upon a new career. Her talk focused upon urinary incontinence (UI).
She separates UI into two general categories, drip type and faucet strength type which is more severe.
When a radical prostatectomy is performed, the portion of the urethra that goes through the prostate is also removed. How much is determined by the size and shape of the prostate. Muscles supporting the bladder are also removed and the bladder is pulled down to compensate for the gland removal. This can cause incontinence. Catheters are normally initially inserted for a time period, but UI issues can linger indefinitely. Radiation causes scar tissue. UI issues will not surface until two to five years later. As men age, they lose core strength, another contributor to UI. Most men are not diagnosed with PCa until they are in their sixties. UI can be present without PCa.
Pressure Flow Tests are performed to determine if the bladder and urinary tract are functioning properly. The test initiates with a full bladder and the patient voids through a catheter. Sensors monitor the function of the urinary tract. The test may involve lying, sitting and standing during the process.
Pelvic Floor Therapy involves specific exercises and aims at strengthening that area of the anatomy and mitigating incontinence issues, primarily dribbling. Some beneficial exercises:
Sara talked about the options for treatment for UI. Some are designed for moderate UI and one in particular is a surgical procedure for severe UI.
Use male designed underwear. She opined that products on the general market, pads and disposable are not favorable. They don't provide proper ventilation, do not prevent odors and don't protect against rash and irritation. She spoke favorably about underwear sold under the "Protechdry" brand.
Sara talked about different types of clamps which prevent urine leakage by pressuring the urethra. They are removable when the urge to void occurs.
Sleeve catheters can cause problems. Urine sits in the bag and can back up into the penile opening. Bruising, rash, irritation and infection can occur.
Botox injections at the base of the bladder help the muscles to relax and be effective in treating mild to moderate UI. They are not permanent and last four to six months.
Urinary sphincters require a surgical procedure. The surgeon places a cuff filled with fluid around the urethra. The surgeon also places a button in the testicles. When the need to void occurs, the patient presses the button, and the fluid is pumped into a reservoir under the bladder for a measured period. If the time limit is not sufficient to empty the bladder, the process can be repeated. This mechanism is like a penile implant whereby when a maa button in the testicles is pushed and fluid is pumped into the penis causing an erection. Different from the sphincter, the man determines when the button is again engaged, draining the fluid from the penis. One man can have both a urinary sphincter and a penile implant since the buttons are on different sides of the testicles. The sphincter button should be placed upon the side of the dominant hand since it will be used more than the penile implant.
Sara mentioned a technique to prevent leakage during sexual function. Sit on the toilet with legs spread as far apart as possible. Place the hands on either side of the belly button with index fingers pointed toward each other. Lean forward and press down causing a urine flow. Hold for a six count. Sit straight up for a six count and then repeat. Do this three times. This exercise can also be useful before bedtime to mitigate nocturia.
Sara talked about penis shrinkage. This happens to a certain extent with age and after an RP. Excess shrinkage can force a man to sit while urinating. Also, the foreskin can cover the penile opening, resulting in poor hygiene. She suggested the use of a vacuum pump regularly to augment blood flow to the penis to mitigate shrinkage and enhance performance. She recommends the Revive Premium System and four erections per week. She warned against acquiring pumps from a porn shop since the quality is often substandard and problems can occur.
Sara mentioned "Scream Cream”. About this time in the presentation, the screen froze, and we did not get a good explanation. Scream Cream is an orgasm enhancer for women.
Sara offers a free 30-minute consultation, and you can get additional information regarding the products that she recommends. You can access her website @ https://www.pivotalrehab.com/ Click on the “Contact Us" menu to register for a consultation.
This presentation was not recorded, primarily because of insurance ramifications. Sara has participated in certain 'podcasts' that you can access by clicking on the "Media" menu on her website.
Fred Barone
[email protected]
Speaker: Sara Sattler, Prostate Cancer Rehab Specialist
Topic: Urinary Incontinence
Our speaker at our hybrid meeting (20 people in the audience and 17 people on Zoom) on September 6 was Sara Sattler. Sara is a Prostate Cancer Rehab Specialist specializing in sexual and intimacy issues and urinary incontinence. She has a technical background in other medical specialties including organ tissue recovery. When her father and father-in-law were diagnosed with PCa, they turned to her for support, and she embarked upon a new career. Her talk focused upon urinary incontinence (UI).
She separates UI into two general categories, drip type and faucet strength type which is more severe.
When a radical prostatectomy is performed, the portion of the urethra that goes through the prostate is also removed. How much is determined by the size and shape of the prostate. Muscles supporting the bladder are also removed and the bladder is pulled down to compensate for the gland removal. This can cause incontinence. Catheters are normally initially inserted for a time period, but UI issues can linger indefinitely. Radiation causes scar tissue. UI issues will not surface until two to five years later. As men age, they lose core strength, another contributor to UI. Most men are not diagnosed with PCa until they are in their sixties. UI can be present without PCa.
Pressure Flow Tests are performed to determine if the bladder and urinary tract are functioning properly. The test initiates with a full bladder and the patient voids through a catheter. Sensors monitor the function of the urinary tract. The test may involve lying, sitting and standing during the process.
Pelvic Floor Therapy involves specific exercises and aims at strengthening that area of the anatomy and mitigating incontinence issues, primarily dribbling. Some beneficial exercises:
- Walking: A low impact exercise that exercises more muscles than any other form of exercise. Walking in place can be performed in one's own home during inclement weather.
- Basic Yoga
- Cigar Kegel. This exercise starts in a sitting position and the individual imagines a cigar is placed between the buttocks. Then the person stands and crunches the buttocks together imagining that he holds the cigar in place. He maintains this position a six count and then slowly releases.
- Turtle Retraction: This involves retracting the head of the penis slowly back to the pelvic area. Imagine a turtle retracting its head back into its shell. Also hold for a six count.
- As one progresses, the hold count can be maintained for up to 15 to 20 seconds.
- Perform 3 in the morning, 3 midday and 3 in the evening of each.
- Hypertonic Pelvic Floor: This is a condition where the muscles in the pelvic area are in a state of spasm or constant contraction. This can be painful and cause urination problems. Medical professional assistance may be necessary.
- Silver Sneakers: The SS website contains several pelvic floor exercises.
Sara talked about the options for treatment for UI. Some are designed for moderate UI and one in particular is a surgical procedure for severe UI.
Use male designed underwear. She opined that products on the general market, pads and disposable are not favorable. They don't provide proper ventilation, do not prevent odors and don't protect against rash and irritation. She spoke favorably about underwear sold under the "Protechdry" brand.
Sara talked about different types of clamps which prevent urine leakage by pressuring the urethra. They are removable when the urge to void occurs.
Sleeve catheters can cause problems. Urine sits in the bag and can back up into the penile opening. Bruising, rash, irritation and infection can occur.
Botox injections at the base of the bladder help the muscles to relax and be effective in treating mild to moderate UI. They are not permanent and last four to six months.
Urinary sphincters require a surgical procedure. The surgeon places a cuff filled with fluid around the urethra. The surgeon also places a button in the testicles. When the need to void occurs, the patient presses the button, and the fluid is pumped into a reservoir under the bladder for a measured period. If the time limit is not sufficient to empty the bladder, the process can be repeated. This mechanism is like a penile implant whereby when a maa button in the testicles is pushed and fluid is pumped into the penis causing an erection. Different from the sphincter, the man determines when the button is again engaged, draining the fluid from the penis. One man can have both a urinary sphincter and a penile implant since the buttons are on different sides of the testicles. The sphincter button should be placed upon the side of the dominant hand since it will be used more than the penile implant.
Sara mentioned a technique to prevent leakage during sexual function. Sit on the toilet with legs spread as far apart as possible. Place the hands on either side of the belly button with index fingers pointed toward each other. Lean forward and press down causing a urine flow. Hold for a six count. Sit straight up for a six count and then repeat. Do this three times. This exercise can also be useful before bedtime to mitigate nocturia.
Sara talked about penis shrinkage. This happens to a certain extent with age and after an RP. Excess shrinkage can force a man to sit while urinating. Also, the foreskin can cover the penile opening, resulting in poor hygiene. She suggested the use of a vacuum pump regularly to augment blood flow to the penis to mitigate shrinkage and enhance performance. She recommends the Revive Premium System and four erections per week. She warned against acquiring pumps from a porn shop since the quality is often substandard and problems can occur.
Sara mentioned "Scream Cream”. About this time in the presentation, the screen froze, and we did not get a good explanation. Scream Cream is an orgasm enhancer for women.
Sara offers a free 30-minute consultation, and you can get additional information regarding the products that she recommends. You can access her website @ https://www.pivotalrehab.com/ Click on the “Contact Us" menu to register for a consultation.
This presentation was not recorded, primarily because of insurance ramifications. Sara has participated in certain 'podcasts' that you can access by clicking on the "Media" menu on her website.
Fred Barone
[email protected]
Monthly Meeting: August 2, 2023
Speaker: Jan Manarite, Executive VP of Cancer ABCs
Topic: What is Nuclear Medicine?
Jan Manarite, Executive VP of Cancer ABCs was our speaker at our meeting on August 2. Forty Seven people attended the meeting. The first part of her presentation was a repeat of a talk she presented to the Society of Nuclear Medicine and Molecular Imaging approximately one month ago titled "What the Heck is Nuclear (in Prostate Cancer?". Jan is a member of that Society's Advisory Board. The second part of her talk was an open forum of questions and answers
Currently Nuclear Medicine (NM) in the USA is both Imaging and Treatment. Imaging consists of Bone Scans (techniciam 99) and any PET scan which includes Axumin (fluciclovine) and PSMA's .(Prostate Specific Membrane Antigen) which include imaging agents Pylarify (pfilufolastat), Illuccix (galium 68) and Poluma (flotufolastat). Treatment agents include Xofigo (radium 223) and Pluvicto (lutetium 177). These agents are considered Radioactive Pharmaceuticals
Regarding Prostate Cancer (PCa) imaging, NM is not MRI's, CT Scans, Dexa
Scans. Ultrasounds, and X-rays. Regarding treatment, NM is not Hormone Therapy, Immunotherapy, Chemotherapy, and External Beam Radiation.
A common misconception is that nuclear medicine is always dangerous. Jan posited a Risk vs. Benefit mindset is important. Another misconception is that NM is always treatment. NM includes both imaging and treatment.
NM imaging can be administered by a NM physician or a radiologist with special training in Nuclear Imaging. NM treatment can be administered by a NM Physician or a Radiation Oncologist. It cannot be administered by an Urologist, Urologiic Oncologist or a Medical Oncologist.
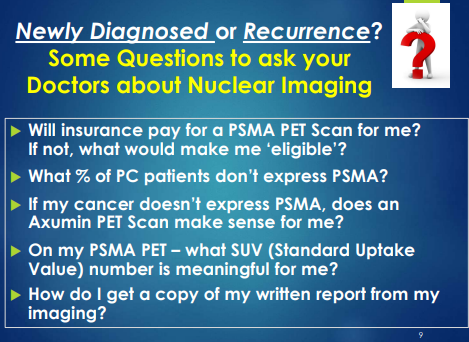
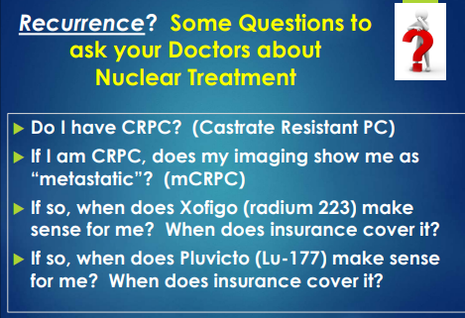
Jan presented two slides regarding questions to ask doctors, one regarding imaging and one regarding treatment.
Speaker: Jan Manarite, Executive VP of Cancer ABCs
Topic: What is Nuclear Medicine?
Jan Manarite, Executive VP of Cancer ABCs was our speaker at our meeting on August 2. Forty Seven people attended the meeting. The first part of her presentation was a repeat of a talk she presented to the Society of Nuclear Medicine and Molecular Imaging approximately one month ago titled "What the Heck is Nuclear (in Prostate Cancer?". Jan is a member of that Society's Advisory Board. The second part of her talk was an open forum of questions and answers
Currently Nuclear Medicine (NM) in the USA is both Imaging and Treatment. Imaging consists of Bone Scans (techniciam 99) and any PET scan which includes Axumin (fluciclovine) and PSMA's .(Prostate Specific Membrane Antigen) which include imaging agents Pylarify (pfilufolastat), Illuccix (galium 68) and Poluma (flotufolastat). Treatment agents include Xofigo (radium 223) and Pluvicto (lutetium 177). These agents are considered Radioactive Pharmaceuticals
Regarding Prostate Cancer (PCa) imaging, NM is not MRI's, CT Scans, Dexa
Scans. Ultrasounds, and X-rays. Regarding treatment, NM is not Hormone Therapy, Immunotherapy, Chemotherapy, and External Beam Radiation.
A common misconception is that nuclear medicine is always dangerous. Jan posited a Risk vs. Benefit mindset is important. Another misconception is that NM is always treatment. NM includes both imaging and treatment.
NM imaging can be administered by a NM physician or a radiologist with special training in Nuclear Imaging. NM treatment can be administered by a NM Physician or a Radiation Oncologist. It cannot be administered by an Urologist, Urologiic Oncologist or a Medical Oncologist.
Jan presented two slides regarding questions to ask doctors, one regarding imaging and one regarding treatment.
|
|
Regarding terminology, Jan advised to Google the big words and discuss the meaning and implications with one's doctor where there is ambiguity.
Questions and Answers:
Who qualifies for PSMA pet scans? Men with suspected recurrence based with elevated PSA levels and men with suspected metastases who are candidates for initial therapy.
What is CRPC? These letters stand for castrate resistant prostate cancer. This is a condition where hormone therapy has basically stopped the production of testosterone but the PCa continues to grow.
An eighty-eight year old gentleman on hormone therapy ( I think Eligard) complained about constant fatigue. He was initially diagnosed 17 years ago and has undergone radiation therapy. His PSA has risen from 1.7 to 3 in somewhat quick succession. His primary care doctor feels that the current therapy is overkill. After a group discussion, the idea to investigate intermittent therapy with a drug similar to Casodex surfaced.
Why do doctors prescribe hormone therapy along with radiation? One reason is the aggressiveness of the PCa. The other reason is to shrink the prostate. Jan stressed the importance of knowing the size of one's prostate. The larger the prostate, the higher the risk of X-ray beams damaging the bladder or the rectum and causing incontinence problems.
She stressed the importance of obtaining one's records for visits and treatments.
One of her slides included her contact information and she is available for one on one questions.
Her presentation is available to view here
Fred Barone
[email protected]
Questions and Answers:
Who qualifies for PSMA pet scans? Men with suspected recurrence based with elevated PSA levels and men with suspected metastases who are candidates for initial therapy.
What is CRPC? These letters stand for castrate resistant prostate cancer. This is a condition where hormone therapy has basically stopped the production of testosterone but the PCa continues to grow.
An eighty-eight year old gentleman on hormone therapy ( I think Eligard) complained about constant fatigue. He was initially diagnosed 17 years ago and has undergone radiation therapy. His PSA has risen from 1.7 to 3 in somewhat quick succession. His primary care doctor feels that the current therapy is overkill. After a group discussion, the idea to investigate intermittent therapy with a drug similar to Casodex surfaced.
Why do doctors prescribe hormone therapy along with radiation? One reason is the aggressiveness of the PCa. The other reason is to shrink the prostate. Jan stressed the importance of knowing the size of one's prostate. The larger the prostate, the higher the risk of X-ray beams damaging the bladder or the rectum and causing incontinence problems.
She stressed the importance of obtaining one's records for visits and treatments.
One of her slides included her contact information and she is available for one on one questions.
Her presentation is available to view here
Fred Barone
[email protected]
Monthly Meeting: June 7, 2023
Speaker: Sara Sattler, Alta Rep, LLS, Pivotal Rehab
Topic: Men's Sexual Health
Our speaker at our hybrid meeting (live audience plus Zoom participants) June 7 with 18 people attending was Sara Sattler, She is a Prostate Cancer Rehab Specialist specializing in sexual and intimacy issues and urinary incontinence. In the meeting, she focused upon sexual and intimacy issues.
Effects of Treatments: After a radical prostatectomy, shrinkage occurs because after the gland is removed, the bladder is pulled down and penile tissue is pulled up to meet the bladder. Urinary incontinence is also common. Sometimes the shrinkage can require the man to sit to urinate into the toilet bowl. These are significant and immediate changes to the male’s composition, like a cut punch. After radiation, the body slowly develops scar tissue that hinders sexual performance. Tiny holes can develop in the penile tissue allowing blood flow to seep out. Restoring blood flow and sensitivity is key.
After treatment Sara recommends meeting with three counselors in three disciplines: 1) a pelvic floor therapist to strengthen the pelvic muscles; 2) at least one visit with a mental health counselor because this is a radical change; 3) consulting with a PA post treatment and letting the urologists and oncologists work on treatments. PA’s are most knowledgeable and sensitive to a patient’s needs.
Sara listed several causes of erectile dysfunction including 1) certain medications (both prescription and over the counter) 2) depression, 3) smoking, 4) excess use of alcohol, 5) other diseases (primarily diabetes and heart disease), and 6) other surgeries. If a man has ED issues before any prostate treatment, he will only recover function to the level prior to the treatment.
There are six primary treatments for ED and Sara presented a slide showing what each looks like.
Mayo Clinic Men’s Health Moment: Penile implant pump
Mayo Men’s Health Moment: Penile Implant Pump Updates
Mayo Clinic Men’s Health Moment: Penile Implant Risks
Shockwave Therapy: This is a procedure that delivers low intensity shockwaves to the penis. This therapy is like the “Wild Wild” West currently, many practitioners from different disciplines. The American Urological Association has not approved this therapy. The National Institute of Health is currently undergoing a massive study. There is a big difference in the quality of the providers.
Women also have sexual dysfunction. Lack of moisture and reduced blood flow can cause pain during sex. Sara recommends buying lubricants in small quantities and avoiding the large quantity containers available in the big box stores. Lubricants can deteriorate over time. Vibration devices are helpful in regaining sensitivity for both men and women.
Here is a link to Sara’s website:
https://www.pivotalrehab.com/
Speaker: Sara Sattler, Alta Rep, LLS, Pivotal Rehab
Topic: Men's Sexual Health
Our speaker at our hybrid meeting (live audience plus Zoom participants) June 7 with 18 people attending was Sara Sattler, She is a Prostate Cancer Rehab Specialist specializing in sexual and intimacy issues and urinary incontinence. In the meeting, she focused upon sexual and intimacy issues.
Effects of Treatments: After a radical prostatectomy, shrinkage occurs because after the gland is removed, the bladder is pulled down and penile tissue is pulled up to meet the bladder. Urinary incontinence is also common. Sometimes the shrinkage can require the man to sit to urinate into the toilet bowl. These are significant and immediate changes to the male’s composition, like a cut punch. After radiation, the body slowly develops scar tissue that hinders sexual performance. Tiny holes can develop in the penile tissue allowing blood flow to seep out. Restoring blood flow and sensitivity is key.
After treatment Sara recommends meeting with three counselors in three disciplines: 1) a pelvic floor therapist to strengthen the pelvic muscles; 2) at least one visit with a mental health counselor because this is a radical change; 3) consulting with a PA post treatment and letting the urologists and oncologists work on treatments. PA’s are most knowledgeable and sensitive to a patient’s needs.
Sara listed several causes of erectile dysfunction including 1) certain medications (both prescription and over the counter) 2) depression, 3) smoking, 4) excess use of alcohol, 5) other diseases (primarily diabetes and heart disease), and 6) other surgeries. If a man has ED issues before any prostate treatment, he will only recover function to the level prior to the treatment.
There are six primary treatments for ED and Sara presented a slide showing what each looks like.
- PDE5 oral medicines, Viagra, and Cialis. These medicines relax the muscle and increase blood flow and combat scar tissue. They work only if one is sexually stimulated, foreplay and touching are important. For PCa patients, these medicines work about 50% of the time. After radical surgery, patients are normally put on these meds not to get erections, but to increase blood flow.
- Injections: Using a diabetic needle, a compound consisting of an irritant to cause an erection, a sensitivity compound and a pain reliever is injected into the penis. The formula can be changed. It is important for patients to communicate with their doctors if problems arise. The patient should inject at 9:00 o’clock and 3 o’clock and alternate sides. In some cases, the man cannot inject himself, then his partner must do so. Side effects can include scarring, infection, and priapism (prolonged erection). To overcome priapism, blood flow must be diverted to other parts of the lower body. Walking, jogging, walking up and down stairs and wall sits are effective. This procedure is not covered by insurance.
- Muse: This is a suppository that is inserted into the opening of the penis. This is not widely used currently and can result in pain, urethral burning, testicular pain, urethral bleeding, and low blood pressure.
- VenoSeal. This is for men who can get erections but can’t maintain them. This is basically a loop that is tightened around the penis to prevent blood from leaking out. A doppler test is available that can show the areas of leakage.
- Vacuum Erection Device (VED); This is a pump that sucks blood into the penis. To keep the blood in the penis, a penile ring is necessary. Rings come in different sizes to fit the particular anatomy and must not be in place for more than 30 minutes. PED5s and VEDs six to eight weeks post op are the safest way to get blood back into the penis and augment size. Sara cautioned the audience to buy an FDA approved VED because it will have a relief valve that will prevent over suction and not to buy one from an adult store. She demonstrated the use of her favorite VED. It comes with a scrotal shield that prevents pubic hair and portions of the scrotum from getting sucked into the vacuum. This device also has a mechanism that facilitates placement of the ring. VEDs can also help in overcoming Peyronie's disease.
- Penile Implants: Fluid is stored in a reservoir in the lower abdomen. Pushing a button in the testicular sac causes the fluid to flow into two tubes on each side of the penis causing an erection. When finished, pressing the button again causes the fluid to drain back into the reservoir. Technology has advanced where there is now an app that can activate the implant procedure. Sara feels that it is important to have a prosthesis specialist perform this surgery, one that performs more than fifty per year. It is important that the implant achieves the proper size and length. Utilization of a VED prior to surgery to stretch the length of the penis facilitates surgery. This is surgery and the risk of infection is always present. Although the penis is engorged, the head of the penis is not affected. A penile implant is the last resort. Once adopted, one can’t go back to the other devices. These implants last on average 15 years and all of Sara’s clients who have implants are extremely happy. An implant and an artificial sphincter can be inserted into the man. One button would be on each side of the scrotal sac. Sara referenced three YouTube videos on implants featuring Dr. Tobias Kohler of the Mayo clinic, here are the links:
Mayo Clinic Men’s Health Moment: Penile implant pump
Mayo Men’s Health Moment: Penile Implant Pump Updates
Mayo Clinic Men’s Health Moment: Penile Implant Risks
Shockwave Therapy: This is a procedure that delivers low intensity shockwaves to the penis. This therapy is like the “Wild Wild” West currently, many practitioners from different disciplines. The American Urological Association has not approved this therapy. The National Institute of Health is currently undergoing a massive study. There is a big difference in the quality of the providers.
Women also have sexual dysfunction. Lack of moisture and reduced blood flow can cause pain during sex. Sara recommends buying lubricants in small quantities and avoiding the large quantity containers available in the big box stores. Lubricants can deteriorate over time. Vibration devices are helpful in regaining sensitivity for both men and women.
Here is a link to Sara’s website:
https://www.pivotalrehab.com/
Monthly Meeting: May 3, 2023
Speaker: Dendreon Representatives
Topic: Provenge Treatment
We had two speakers at our virtual meeting on Wednesday on May 3. Dr. Damien Sorce, urologist affiliated with Colorado Urology Associates and advocate Mr. Euvon Jones. Additionally several representatives of Dendreon attended. Dendreon provides Provenge, an immunotherapy product.
Dr. Sorce practices general urology but focuses on prostate cancer (PCa). He specializes in minimally invasive urological surgeries. His goal for his talk is three fold: 1) for all people in the audience to be advocates for PCa. The earlier one discovers the disease the better; 2) for attendees to be advocates for men who have not learned to live with PCa. Attendees are members of a support group and have learned to live with PCa. Many men do not have a support network. and 3) to talk about the immune system, immunotherapy and Provenge. Provenge is a immunotherapy approved by the FDA. The procedure extracts immune cells from the body and then treats them with interleukins and cytokines. The immune cells are reinjected into the body and can recognize the cancer mutations and attack them.
Euvon Jones is an advocate who is living with PCa. He shared his journey, diagnosis, treatment, side effects, lifestyle changes, faith.
Speaker: Dendreon Representatives
Topic: Provenge Treatment
We had two speakers at our virtual meeting on Wednesday on May 3. Dr. Damien Sorce, urologist affiliated with Colorado Urology Associates and advocate Mr. Euvon Jones. Additionally several representatives of Dendreon attended. Dendreon provides Provenge, an immunotherapy product.
Dr. Sorce practices general urology but focuses on prostate cancer (PCa). He specializes in minimally invasive urological surgeries. His goal for his talk is three fold: 1) for all people in the audience to be advocates for PCa. The earlier one discovers the disease the better; 2) for attendees to be advocates for men who have not learned to live with PCa. Attendees are members of a support group and have learned to live with PCa. Many men do not have a support network. and 3) to talk about the immune system, immunotherapy and Provenge. Provenge is a immunotherapy approved by the FDA. The procedure extracts immune cells from the body and then treats them with interleukins and cytokines. The immune cells are reinjected into the body and can recognize the cancer mutations and attack them.
Euvon Jones is an advocate who is living with PCa. He shared his journey, diagnosis, treatment, side effects, lifestyle changes, faith.
Monthly Meeting: April 5, 2023
Speaker: Dr. John Dibianco, Urologist, University of Florida Health, Gainesville
Topic: Urologic/Prostate Diagnosis and Treatment
No Transcript available
Speaker: Dr. John Dibianco, Urologist, University of Florida Health, Gainesville
Topic: Urologic/Prostate Diagnosis and Treatment
No Transcript available
Monthly Meeting: March 1, 2023
Speaker: Dr. Tracy Gapin, MD F.A.C.S. Urologist
Topic: Testosterone and Health
Dr. Tracy Gapin was our speaker via Zoom on March 1. Thirty seven people attended, 17 on Zoom and 20 in person. Dr. Gapin is a Board Certified Urologist. For over twenty years, Dr. Gapin was involved with a successful urological surgery practice. During that time he did not enjoy a healthy lifestyle. and subsequently gave up his successful practice to form the Gapin Institute to promote High Performance Health. Hormone management, including testosterone, is a key factor in this philosophy. We recorded his presentation but a summary of his talk is not available.
Speaker: Dr. Tracy Gapin, MD F.A.C.S. Urologist
Topic: Testosterone and Health
Dr. Tracy Gapin was our speaker via Zoom on March 1. Thirty seven people attended, 17 on Zoom and 20 in person. Dr. Gapin is a Board Certified Urologist. For over twenty years, Dr. Gapin was involved with a successful urological surgery practice. During that time he did not enjoy a healthy lifestyle. and subsequently gave up his successful practice to form the Gapin Institute to promote High Performance Health. Hormone management, including testosterone, is a key factor in this philosophy. We recorded his presentation but a summary of his talk is not available.
Monthly Meeting: Jan 4, 2023
Speaker: Dr. Michael Greenberg of Jefferson Health in Philadelphia ( Previously Recorded Video)
Topic: The Future of Radiation in Prostate Cancer
We did not have a speaker for our meeting Wednesday, Jan. 4. We played a video :"The Future of Radiation in Prostate Cancer." The speaker on the Video is Dr. Michael Greenberg, Clinical Associate Professor and Vice Chair of Business Development Radiation Oncology at Jefferson Health in Philadelphia. Dr. Greenberg is part of the Myriad Genetics advisory board involved with implementation of biomarkers in the treatment of prostate cancer (PCa). Additionally, he has been working with Boston Scientific on their SpaceOAR program.
He started his talk with a review of basic statistics of PCa, 248,000 men diagnosed annually, 34,000 deaths annually and 3.1 million men living with PCa. He talked about prostate anatomy, the different types of PCas, risk factors, gene changes, and recommendations for early detection,
Radiation is delivered by linear accelerators. A recent innovation was the introduction of a linear accelerator built into an MRI machine. This allows radiation oncologists to track the motion of the prostate while delivering treatment. This device is known as the MRIdian. As the prostate moves outside a predefined target area, the machine shuts off until the prostate moves back inside the area.
Dr. presented several images comparing the images from an MRI to CT scan images.clearly showing the benefits of an MRI image.
He then showed a video of an actual radiation treatment of the prostate using the MRIdian device. The really informative aspect of this video is the movement of the prostate from breathing, the flow of urine into the bladder and the flow of bowel gas through the intestines.
With this technology, radiation treatments can target tumors as small as one or two millimeters. Dr. Greenberg's facility will also provide radiation treatments to patients who have had previous radiation therapy. Jefferson has an active re-treatment facility. There are fifty six centers worldwide that have this device. Cancer centers in Florida are 1) Moffitt Cancer in Tampa, 2) Orlando Health Cancer Institute and 3) Miami Cancer Institute. ViewRay Inc. manufactures this device. You can visit their website, https://viewray.com/ for more information.
Dr. Greenberg then talked about PSMA Pet Scans. PET scans rely on metabolic imaging using sugar to define the target. PSMA Pet scans can identify very small metastases and radiology oncologists can treat oligometastases with high doses before the cancer can spread.
The typical patient is someone who has been treated for prostate cancer. Their PSA is near zero and then starts to rise. Practitioners know that the images that light up are recurrent disease because they are specific to the PSA molecule.
Dr. presented PSMA Pet images of several patients, pointed out what the images meant and discussed the treatment. Dr. Greenberg uses the MRI linear accelerator to treat with high dosages of radiation, Normally 5 fractions are sufficient. The exactness of the MRI linear accelerator allows treatment of these small metastases.
Dr. Greenberg then discussed SpaceOAR, introduced in 2016, which is a hydrogel inserted between the rectum and the prostate to provide a barrier preventing radiation rays from approaching the rectum. At Jefferson, Dr. uses a new revolutionary gel, Barrigel. Barrigel is made from hyaluronic acid. This gel allows practitioners to sculpt the insertion providing a custom fit. This gel does not get as hard as the original gel.
With the MRI linear accelerator, practitioners can offer treatment to small, recurrent metastases in the prostate bed after a radical prostatectomy.
Dr. Greenberg's facility also uses Lutetium 177 to treat metastatic PCa where appropriate. This radionuclide is an improvement over the prior standard of Radium 223.
To view this video, access the following link and scroll down to "The Future of Radiation in Prostate Cancer."
The Future of Radiation in Prostate Cancer
Fred Barone
[email protected]
Speaker: Dr. Michael Greenberg of Jefferson Health in Philadelphia ( Previously Recorded Video)
Topic: The Future of Radiation in Prostate Cancer
We did not have a speaker for our meeting Wednesday, Jan. 4. We played a video :"The Future of Radiation in Prostate Cancer." The speaker on the Video is Dr. Michael Greenberg, Clinical Associate Professor and Vice Chair of Business Development Radiation Oncology at Jefferson Health in Philadelphia. Dr. Greenberg is part of the Myriad Genetics advisory board involved with implementation of biomarkers in the treatment of prostate cancer (PCa). Additionally, he has been working with Boston Scientific on their SpaceOAR program.
He started his talk with a review of basic statistics of PCa, 248,000 men diagnosed annually, 34,000 deaths annually and 3.1 million men living with PCa. He talked about prostate anatomy, the different types of PCas, risk factors, gene changes, and recommendations for early detection,
Radiation is delivered by linear accelerators. A recent innovation was the introduction of a linear accelerator built into an MRI machine. This allows radiation oncologists to track the motion of the prostate while delivering treatment. This device is known as the MRIdian. As the prostate moves outside a predefined target area, the machine shuts off until the prostate moves back inside the area.
Dr. presented several images comparing the images from an MRI to CT scan images.clearly showing the benefits of an MRI image.
He then showed a video of an actual radiation treatment of the prostate using the MRIdian device. The really informative aspect of this video is the movement of the prostate from breathing, the flow of urine into the bladder and the flow of bowel gas through the intestines.
With this technology, radiation treatments can target tumors as small as one or two millimeters. Dr. Greenberg's facility will also provide radiation treatments to patients who have had previous radiation therapy. Jefferson has an active re-treatment facility. There are fifty six centers worldwide that have this device. Cancer centers in Florida are 1) Moffitt Cancer in Tampa, 2) Orlando Health Cancer Institute and 3) Miami Cancer Institute. ViewRay Inc. manufactures this device. You can visit their website, https://viewray.com/ for more information.
Dr. Greenberg then talked about PSMA Pet Scans. PET scans rely on metabolic imaging using sugar to define the target. PSMA Pet scans can identify very small metastases and radiology oncologists can treat oligometastases with high doses before the cancer can spread.
The typical patient is someone who has been treated for prostate cancer. Their PSA is near zero and then starts to rise. Practitioners know that the images that light up are recurrent disease because they are specific to the PSA molecule.
Dr. presented PSMA Pet images of several patients, pointed out what the images meant and discussed the treatment. Dr. Greenberg uses the MRI linear accelerator to treat with high dosages of radiation, Normally 5 fractions are sufficient. The exactness of the MRI linear accelerator allows treatment of these small metastases.
Dr. Greenberg then discussed SpaceOAR, introduced in 2016, which is a hydrogel inserted between the rectum and the prostate to provide a barrier preventing radiation rays from approaching the rectum. At Jefferson, Dr. uses a new revolutionary gel, Barrigel. Barrigel is made from hyaluronic acid. This gel allows practitioners to sculpt the insertion providing a custom fit. This gel does not get as hard as the original gel.
With the MRI linear accelerator, practitioners can offer treatment to small, recurrent metastases in the prostate bed after a radical prostatectomy.
Dr. Greenberg's facility also uses Lutetium 177 to treat metastatic PCa where appropriate. This radionuclide is an improvement over the prior standard of Radium 223.
To view this video, access the following link and scroll down to "The Future of Radiation in Prostate Cancer."
The Future of Radiation in Prostate Cancer
Fred Barone
[email protected]
Disclaimer: The Villages Prostate Group does not recommend or endorse the speakers, publications or descriptions of publications. They are simply provided as additional resources for your information.
