Speaker Summaries (2022)
Monthly Meeting: December 7, 2022
Speaker: Dr. Mathew Allaway MD, Osteopathic Medicine (OD)
Topic: Precision Point Transperineal Access System
Dr. Mathew Allaway spoke to us via Zoom on December 7 to a joint live audience and Zoom participants, Dr. Allaway is a urologist having his training at Chicago College of Osteopathy. He has over twenty years’ experience and has invented the Precision Point Transperineal Access System. In the 2012 time-frame he came to a crossroads in his practice. Many of his patients were properly engaging in Active Surveillance while others were under-diagnosed because of inadequate Transrectal Biopsies (TR). He decided never to do a TR again and opted for Transperineal biopsies (TP).
Key Statistics:
He showed some MRI graphics and expressed the opinion that all men should be offered an MRI before undergoing a biopsy. Dr. wants the audience to understand that there are several different zones in the prostate, peripheral, transitional, anterior, central and seminal vesicles all packed together. The challenge in performing a biopsy is to find out where the cancer is hiding.
The first prostate biopsy (PBx) was performed in 1926 and entrance was through the perineum. The prostate was opened, tissue extracted and if cancer was likely a partial or total prostatectomy was performed. The procedure required general anesthesia and a week post op hospital stay. Up until the late 1960's several different needle approaches were introduced, but entry was always through the perineum.
In the early 1980's the development of ultrasound technology provided the ability to view the prostate by probing through the rectum. Prior to this technology, PBx was performed using palpation to determine where to insert the probe through the perineum. Urologists at that time did not understand that they could use ultrasound equipment to insert the probe through the perineum.
In 1986, the FDA approved the PSA test that allowed practitioners to suspect PCa before feeling it.
Two major problems developed with the utilization of TR. The first is infection. due to fluoroquinolone-resistant bacteria. TR cannot be done without antibiotics, but the problem is that the bacteria develop strains resistant to antibiotics. The second problem was under diagnosis. Up to 30% of the cancers were missing with the traditional 12 core TR.
There are two approaches to combating infections. In the "Smart Bomb" or targeted approach, swabs are taken to determine the type of bacteria and if resistant to the standard antibiotic, the approached bombarded the patient with a different antibiotic. The other approach was the 'Shotgun” or Augmented approach pumping the patient with several different antibiotics. Pump the patient with everything and something will stick. Both approaches reduce the risk of sepsis but do not eliminate it.
The next slide showed a graphic of a TR which showed the needle going through the rectal wall and introducing fecal material into the prostate.
An Australian study of 7,000 men having TP Bxs revealed only 5 infections, almost zero.
A graphic reflected a study performed by Sloan Kettering Cancer center. It showed that TR missed cancers in the anterior and the apex. TR cannot access these areas of the prostate.
TP is not standard because of the equipment used to perform them. The Grid Stepper Stabilizer is a big bulky piece of equipment. The procedure is expensive, difficult to perform, requires general anesthesia, and complications include pain and perineal swelling and urine retention. The procedure utilizes a grid plate that is placed against the perineum with 169 potential entry points. The biopsy gun can be placed through every hole and the practitioner takes samples in rows and columns normally taking 40 to 50 samples.
Dr. Allaway determined that a different approach was necessary. The performance standard not only needed a different device, but also a different technique that 1) could be performed under local anesthesia through two simple skin punctures, 2) required both time and resources comparable to TR, 3) would eliminate complications, 4) would eliminate bowel preparation and antibiotics, and 5) provide complete prostate anatomy access to optimize cancer detection.
The next slide showed a picture of the Precision Point Device which is a freehand piece of equipment. In the United Kingdom, 80% of all PBxs utilize the Precision Point System (PPS). The European Association of Urology has changed their guidelines and endorsed the PPS as the preferred method of performing PBx. The American Urological Association (AUA) has endorsed the benefits of the TP approach but have not changed their guidelines.
Dr. Allaway presented a graph from a European Meta-Analysis that showed that infections were dramatically lower with TP vs. TR biopsies. He then presented a graph comparing hospitalization rates and sepsis rates in Europe, North America and Asia, TP vs. TR. Basically, the same results as the European study.
Doctor then presented a schematic showing the results of a study done in Israel. The study compared fusion TP vs. fusion TR. In the study, the procedure started with fusion TR, and they switched to fusion TP in the same patient. The results showed a significantly higher degree of detection with TP, deflating the argument that fusion TR is as good as fusion TP. Also, the amount of cancer found per core was better with TP, less cores to get a better overall substance of cancer.
The next schematic presented came from a study in Italy comparing fusion TR with cognitive TP in the same patient. Here again the study found a higher incidence of cancer with TP and a higher concentration per core.
Study results from a 2021 Johns Hopkins study compared TR fusion with TP cognitive base upon MRI PiRad scores for men on Active Surveillance. Fusion technology was not available for TP at the time of the study but now it is. For men with PiRad 3 scores, 28% were upgraded to Grade Group (GG) 2 under TP compared to 14% under TR. For men with PiRad 4 scores, 45% were upgraded to GG2 under TP compared to 28% under TR. Men were better served and properly classified with TP compared to TR.
Dr. Mathew presented slides summarizing two more studies, (one from MD Anderson) and the studies showed TP outperforming TR.
TP biopsies utilizing PPS technology can be performed under local anesthesia. Dr. opined that he local anesthesia is appropriate for 85% of patients but there are 10 to 15% that should have general anesthesia. He cited studies where TP pain experience under local anesthesia was no worse than TR.
Dr. then reported on a study to determine the feasibility of eliminating antibiotics when performing TP. 500 men were given one shot of cephazolin, and 500 men did not receive any antibiotics. There were no documented infections in the prophylaxis group and two culture documented infections in the no prophylaxis group. No patient required hospital admission or was managed with oral biotics. One patient in the no prophylaxis group required a catheter for urine retention.
Dr. Allaway opined that PPS is becoming the standard for TP biopsies. A key feature of PPS is that there are only two needle sticks in the body. The methodology includes a very specific nerve block. The key bolus of Lidocaine is injected in the middle of the pelvic floor muscle. This allows the procedure to be done in the physician's office under local anesthesia. Dr. presented a picture showing the path of the nerve block and then a picture of the template one follows performing the procedure.
Dr. then presented a video of the actual procedure, showing both the internal image and where the samples are taken and an external view showing the placement of the device and how it accesses the perineum. If the procedure is performed under local anesthesia, the patient can drive himself both to and from the doctor's office. There normally is a small amount of blood in the urine but not enough to be concerned with. There will be an impressive amount of blood in the ejaculate. This is to be expected because the procedure takes biopsies from the seminal vesicles in order to cover the entire anatomy.
TP biopsies have become standard procedure using PPS or are in the process of becoming standard procedure, at Johns Hopkins, Mayo Clinic, Cleveland Clinic, Mass General, and Stanford. Adoption of the PPS procedure is beginning to trickle down into local practitioners. To acquire PPS, doctors must be certified competent by Dr. Alloway or one of his staff. To find a practitioner in your area, go to this website and scroll down to the bottom of the page and either fill out the form or contact them by phone or email.
https://perineologic.com/aboutpl-2/
Questions:
How does the PPS relate to PSMA Pet scans? PSMA Pet scans are not approved by the FDA prior to biopsy. They cost $6,000 to $7,000 and insurance companies are strict, normally approving them for patients who have had treatment that has failed. Sometimes they will be approved after biopsy in order to get a more accurate diagnosis.
Will PSMA eventually replace a biopsy? Dr. doesn't believe so. PSMA does not work well for patients with Gleason 3+3. You can't get a PSMA Pet scan, find the patient has cancer, and say let's treat it. You need to obtain tissue to determine the severity of the cancer and the appropriateness of active surveillance
What percentage of biopsies are done using PPS? This is hard to determine because the billing code for biopsies is generic and does not identify the type of biopsy performed. Based upon his sales data, Dr. estimates about 5%, but usage is accelerating rapidly.
How appropriate is PPS for very large prostates requiring forty cores or more? Dr. never used the Grid Stripper device because it required forty to fifty cores resulting in excessive trauma to the prostate. The bigger the prostate, the lower the cores. The transitional zone hogs up most of the prostate and compresses the peripheral and anterior zones. There is less real estate to sample. With PPS, it is not necessary to take medication to shrink the prostate because PPS can access all zones regardless of size.
Fusion biopsies are now available with PPS. What type of MRI equipment should be used? Ideally a 3T MRI should be used. It is not just the equipment, but also the competency of the radiologist reading the MRI. Be selective in choosing an MRI center.
Fred Barone
[email protected]
Speaker: Dr. Mathew Allaway MD, Osteopathic Medicine (OD)
Topic: Precision Point Transperineal Access System
Dr. Mathew Allaway spoke to us via Zoom on December 7 to a joint live audience and Zoom participants, Dr. Allaway is a urologist having his training at Chicago College of Osteopathy. He has over twenty years’ experience and has invented the Precision Point Transperineal Access System. In the 2012 time-frame he came to a crossroads in his practice. Many of his patients were properly engaging in Active Surveillance while others were under-diagnosed because of inadequate Transrectal Biopsies (TR). He decided never to do a TR again and opted for Transperineal biopsies (TP).
Key Statistics:
- Approximately 248,000 thousand new cases per year and 34,000 deaths
- About 1.7 - 1.9 million biopsies performed in the US each year and 3 million worldwide
- 1/8 men will be diagnosed in their lifetimes
He showed some MRI graphics and expressed the opinion that all men should be offered an MRI before undergoing a biopsy. Dr. wants the audience to understand that there are several different zones in the prostate, peripheral, transitional, anterior, central and seminal vesicles all packed together. The challenge in performing a biopsy is to find out where the cancer is hiding.
The first prostate biopsy (PBx) was performed in 1926 and entrance was through the perineum. The prostate was opened, tissue extracted and if cancer was likely a partial or total prostatectomy was performed. The procedure required general anesthesia and a week post op hospital stay. Up until the late 1960's several different needle approaches were introduced, but entry was always through the perineum.
In the early 1980's the development of ultrasound technology provided the ability to view the prostate by probing through the rectum. Prior to this technology, PBx was performed using palpation to determine where to insert the probe through the perineum. Urologists at that time did not understand that they could use ultrasound equipment to insert the probe through the perineum.
In 1986, the FDA approved the PSA test that allowed practitioners to suspect PCa before feeling it.
Two major problems developed with the utilization of TR. The first is infection. due to fluoroquinolone-resistant bacteria. TR cannot be done without antibiotics, but the problem is that the bacteria develop strains resistant to antibiotics. The second problem was under diagnosis. Up to 30% of the cancers were missing with the traditional 12 core TR.
There are two approaches to combating infections. In the "Smart Bomb" or targeted approach, swabs are taken to determine the type of bacteria and if resistant to the standard antibiotic, the approached bombarded the patient with a different antibiotic. The other approach was the 'Shotgun” or Augmented approach pumping the patient with several different antibiotics. Pump the patient with everything and something will stick. Both approaches reduce the risk of sepsis but do not eliminate it.
The next slide showed a graphic of a TR which showed the needle going through the rectal wall and introducing fecal material into the prostate.
An Australian study of 7,000 men having TP Bxs revealed only 5 infections, almost zero.
A graphic reflected a study performed by Sloan Kettering Cancer center. It showed that TR missed cancers in the anterior and the apex. TR cannot access these areas of the prostate.
TP is not standard because of the equipment used to perform them. The Grid Stepper Stabilizer is a big bulky piece of equipment. The procedure is expensive, difficult to perform, requires general anesthesia, and complications include pain and perineal swelling and urine retention. The procedure utilizes a grid plate that is placed against the perineum with 169 potential entry points. The biopsy gun can be placed through every hole and the practitioner takes samples in rows and columns normally taking 40 to 50 samples.
Dr. Allaway determined that a different approach was necessary. The performance standard not only needed a different device, but also a different technique that 1) could be performed under local anesthesia through two simple skin punctures, 2) required both time and resources comparable to TR, 3) would eliminate complications, 4) would eliminate bowel preparation and antibiotics, and 5) provide complete prostate anatomy access to optimize cancer detection.
The next slide showed a picture of the Precision Point Device which is a freehand piece of equipment. In the United Kingdom, 80% of all PBxs utilize the Precision Point System (PPS). The European Association of Urology has changed their guidelines and endorsed the PPS as the preferred method of performing PBx. The American Urological Association (AUA) has endorsed the benefits of the TP approach but have not changed their guidelines.
Dr. Allaway presented a graph from a European Meta-Analysis that showed that infections were dramatically lower with TP vs. TR biopsies. He then presented a graph comparing hospitalization rates and sepsis rates in Europe, North America and Asia, TP vs. TR. Basically, the same results as the European study.
Doctor then presented a schematic showing the results of a study done in Israel. The study compared fusion TP vs. fusion TR. In the study, the procedure started with fusion TR, and they switched to fusion TP in the same patient. The results showed a significantly higher degree of detection with TP, deflating the argument that fusion TR is as good as fusion TP. Also, the amount of cancer found per core was better with TP, less cores to get a better overall substance of cancer.
The next schematic presented came from a study in Italy comparing fusion TR with cognitive TP in the same patient. Here again the study found a higher incidence of cancer with TP and a higher concentration per core.
Study results from a 2021 Johns Hopkins study compared TR fusion with TP cognitive base upon MRI PiRad scores for men on Active Surveillance. Fusion technology was not available for TP at the time of the study but now it is. For men with PiRad 3 scores, 28% were upgraded to Grade Group (GG) 2 under TP compared to 14% under TR. For men with PiRad 4 scores, 45% were upgraded to GG2 under TP compared to 28% under TR. Men were better served and properly classified with TP compared to TR.
Dr. Mathew presented slides summarizing two more studies, (one from MD Anderson) and the studies showed TP outperforming TR.
TP biopsies utilizing PPS technology can be performed under local anesthesia. Dr. opined that he local anesthesia is appropriate for 85% of patients but there are 10 to 15% that should have general anesthesia. He cited studies where TP pain experience under local anesthesia was no worse than TR.
Dr. then reported on a study to determine the feasibility of eliminating antibiotics when performing TP. 500 men were given one shot of cephazolin, and 500 men did not receive any antibiotics. There were no documented infections in the prophylaxis group and two culture documented infections in the no prophylaxis group. No patient required hospital admission or was managed with oral biotics. One patient in the no prophylaxis group required a catheter for urine retention.
Dr. Allaway opined that PPS is becoming the standard for TP biopsies. A key feature of PPS is that there are only two needle sticks in the body. The methodology includes a very specific nerve block. The key bolus of Lidocaine is injected in the middle of the pelvic floor muscle. This allows the procedure to be done in the physician's office under local anesthesia. Dr. presented a picture showing the path of the nerve block and then a picture of the template one follows performing the procedure.
Dr. then presented a video of the actual procedure, showing both the internal image and where the samples are taken and an external view showing the placement of the device and how it accesses the perineum. If the procedure is performed under local anesthesia, the patient can drive himself both to and from the doctor's office. There normally is a small amount of blood in the urine but not enough to be concerned with. There will be an impressive amount of blood in the ejaculate. This is to be expected because the procedure takes biopsies from the seminal vesicles in order to cover the entire anatomy.
TP biopsies have become standard procedure using PPS or are in the process of becoming standard procedure, at Johns Hopkins, Mayo Clinic, Cleveland Clinic, Mass General, and Stanford. Adoption of the PPS procedure is beginning to trickle down into local practitioners. To acquire PPS, doctors must be certified competent by Dr. Alloway or one of his staff. To find a practitioner in your area, go to this website and scroll down to the bottom of the page and either fill out the form or contact them by phone or email.
https://perineologic.com/aboutpl-2/
Questions:
How does the PPS relate to PSMA Pet scans? PSMA Pet scans are not approved by the FDA prior to biopsy. They cost $6,000 to $7,000 and insurance companies are strict, normally approving them for patients who have had treatment that has failed. Sometimes they will be approved after biopsy in order to get a more accurate diagnosis.
Will PSMA eventually replace a biopsy? Dr. doesn't believe so. PSMA does not work well for patients with Gleason 3+3. You can't get a PSMA Pet scan, find the patient has cancer, and say let's treat it. You need to obtain tissue to determine the severity of the cancer and the appropriateness of active surveillance
What percentage of biopsies are done using PPS? This is hard to determine because the billing code for biopsies is generic and does not identify the type of biopsy performed. Based upon his sales data, Dr. estimates about 5%, but usage is accelerating rapidly.
How appropriate is PPS for very large prostates requiring forty cores or more? Dr. never used the Grid Stripper device because it required forty to fifty cores resulting in excessive trauma to the prostate. The bigger the prostate, the lower the cores. The transitional zone hogs up most of the prostate and compresses the peripheral and anterior zones. There is less real estate to sample. With PPS, it is not necessary to take medication to shrink the prostate because PPS can access all zones regardless of size.
Fusion biopsies are now available with PPS. What type of MRI equipment should be used? Ideally a 3T MRI should be used. It is not just the equipment, but also the competency of the radiologist reading the MRI. Be selective in choosing an MRI center.
Fred Barone
[email protected]
Monthly Meeting: October 5, 2022
Speaker: Dr. Nicholas Maruniak, MD, Board Certified Pathologist, Advanced Urological Institute.
Topic: Prostate Pathology
Our speaker on October 5 was Dr. Nicholas Maruniak. He is currently an active pathologist and practices with Advanced Urological Institute. He is Certified by the American Board of Pathology in Anatomic and Clinical Pathology. Dr. Marunial is a member of the American Society for clinical Pathology and the International Society of Urological Pathology.
How Cancer Develops: Cells in the body normally are programmed to stop or slow down growing when they come in contact with another cell. This is called contact inhibition. One of the first changes that happens when a cell turns malignant is loss of contact inhibition. Cells begin piling up and may start to grow where they shouldn’t (form a mass and invade).
Adenocarcinoma is the type of cancer that develops in gland cells. It is the most common type of cancer found in the prostate gland. Glandular cells are usually involved in secreting or absorbing substances.
Pathologists grade prostate cancers with the Gleason system using numbers from 1 to 5 based on how much the cells in the cancerous tissue look like normal prostate tissue under the microscope (Gleason pattern).
Gleason patterns 1 and 2 are not used any more for biopsies. Most biopsy samples are pattern 3, 4 or 5. If the cancerous tissue looks much like normal prostate tissue, pattern 3 is assigned. If the cancer cells and their growth patterns look very abnormal, pattern 5 is assigned. Since prostate cancers often have areas with different patterns, a pattern number is assigned to the 2 areas that make up most of the cancer. These 2 pattern numbers are added to give the Gleason score. The highest a Gleason score can be is 10. The first number assigned is the pattern that is most common in the tumor. For example, if the Gleason score is written as 3+4=7, it means most of the tumor is pattern 3 and less is pattern 4, and they are added for a Gleason score of 7. The higher the Gleason score, the more likely it is that your cancer will grow and spread quickly
The Gleason score is very important in predicting the behavior of prostate cancer and determining the best treatment options. However other factors are important including, the blood PSA level, findings on a rectal exam, findings on imaging tests, the number of cores with cancer and how much of each core is made up of cancer, whether cancer is found on both sides of the prostate and whether the cancer has spread outside the prostate. Taken together all these factors what risk group the cancer falls into, very low risk, low risk, favorable intermediate, unfavorable intermediate, high risk and very high risk.
Grade groups are a new way to grade prostate cancer to address the issues with the Gleason grading system. Gleason 6 is the lowest Gleason score, but it might lead some patients to think that they are in the middle of the grade scale.
Grade Group 1 = Gleason 6
Grade Group 2 = Gleason 3+4.
Grade Group 3 = Gleason 4+3
Grade Group 4 = Gleason 4+4
Grade Group 5 = Gleason 9-1
Hazard Ratio: The groups are correlated with a Hazard Ratio that reflect the risk of PSA rising relative to a Gleason 6. There is a significant difference between Grade Group 2 and Grade Group 3.
Grade Group 1 Gleason 6 1
Grade Group 2 Gleason 3+4 1.9
Grade Group 3 Gleason 4+3 5.1
Grade Group 4 Gleason 8 8.0
Grade Group 5 Gleason 9&10' 11.7
Dr. Maruniak then presented several slides showing biopsies of the prostate ranging from a normal prostate up to Grade Group 5. He explained what the slides reflected; however, I am not including the slides in this summary.
Other Comments:
A normal biopsy samples approximately one one thousandth of the prostate gland.
His practice keeps biopsy reports for 20 years and the paraffin block containing the tissue for 10 years.
A saturated biopsy may contain 20 up to 60 cores, one core for every gram. These biopsies are performed when PSA's are rising but normal twelve core biopsy shows no results. The higher the cores taken, the higher the risk of damage to the gland.
Dr. Maruniak wil give second opinions on biopsies performed outside the AUI practice. He mentioned Joel Epstein of Johns Hopkins as a pathologist who does multiple second opinions'
In a Gleason 3+4 biopsy report, Dr. Maruniak does not publish the percentage of Gleason 3 vs. Gleason 4. Such percentages are too subjective.
Fred Barone
[email protected]
Speaker: Dr. Nicholas Maruniak, MD, Board Certified Pathologist, Advanced Urological Institute.
Topic: Prostate Pathology
Our speaker on October 5 was Dr. Nicholas Maruniak. He is currently an active pathologist and practices with Advanced Urological Institute. He is Certified by the American Board of Pathology in Anatomic and Clinical Pathology. Dr. Marunial is a member of the American Society for clinical Pathology and the International Society of Urological Pathology.
How Cancer Develops: Cells in the body normally are programmed to stop or slow down growing when they come in contact with another cell. This is called contact inhibition. One of the first changes that happens when a cell turns malignant is loss of contact inhibition. Cells begin piling up and may start to grow where they shouldn’t (form a mass and invade).
Adenocarcinoma is the type of cancer that develops in gland cells. It is the most common type of cancer found in the prostate gland. Glandular cells are usually involved in secreting or absorbing substances.
Pathologists grade prostate cancers with the Gleason system using numbers from 1 to 5 based on how much the cells in the cancerous tissue look like normal prostate tissue under the microscope (Gleason pattern).
Gleason patterns 1 and 2 are not used any more for biopsies. Most biopsy samples are pattern 3, 4 or 5. If the cancerous tissue looks much like normal prostate tissue, pattern 3 is assigned. If the cancer cells and their growth patterns look very abnormal, pattern 5 is assigned. Since prostate cancers often have areas with different patterns, a pattern number is assigned to the 2 areas that make up most of the cancer. These 2 pattern numbers are added to give the Gleason score. The highest a Gleason score can be is 10. The first number assigned is the pattern that is most common in the tumor. For example, if the Gleason score is written as 3+4=7, it means most of the tumor is pattern 3 and less is pattern 4, and they are added for a Gleason score of 7. The higher the Gleason score, the more likely it is that your cancer will grow and spread quickly
The Gleason score is very important in predicting the behavior of prostate cancer and determining the best treatment options. However other factors are important including, the blood PSA level, findings on a rectal exam, findings on imaging tests, the number of cores with cancer and how much of each core is made up of cancer, whether cancer is found on both sides of the prostate and whether the cancer has spread outside the prostate. Taken together all these factors what risk group the cancer falls into, very low risk, low risk, favorable intermediate, unfavorable intermediate, high risk and very high risk.
Grade groups are a new way to grade prostate cancer to address the issues with the Gleason grading system. Gleason 6 is the lowest Gleason score, but it might lead some patients to think that they are in the middle of the grade scale.
Grade Group 1 = Gleason 6
Grade Group 2 = Gleason 3+4.
Grade Group 3 = Gleason 4+3
Grade Group 4 = Gleason 4+4
Grade Group 5 = Gleason 9-1
Hazard Ratio: The groups are correlated with a Hazard Ratio that reflect the risk of PSA rising relative to a Gleason 6. There is a significant difference between Grade Group 2 and Grade Group 3.
Grade Group 1 Gleason 6 1
Grade Group 2 Gleason 3+4 1.9
Grade Group 3 Gleason 4+3 5.1
Grade Group 4 Gleason 8 8.0
Grade Group 5 Gleason 9&10' 11.7
Dr. Maruniak then presented several slides showing biopsies of the prostate ranging from a normal prostate up to Grade Group 5. He explained what the slides reflected; however, I am not including the slides in this summary.
Other Comments:
A normal biopsy samples approximately one one thousandth of the prostate gland.
His practice keeps biopsy reports for 20 years and the paraffin block containing the tissue for 10 years.
A saturated biopsy may contain 20 up to 60 cores, one core for every gram. These biopsies are performed when PSA's are rising but normal twelve core biopsy shows no results. The higher the cores taken, the higher the risk of damage to the gland.
Dr. Maruniak wil give second opinions on biopsies performed outside the AUI practice. He mentioned Joel Epstein of Johns Hopkins as a pathologist who does multiple second opinions'
In a Gleason 3+4 biopsy report, Dr. Maruniak does not publish the percentage of Gleason 3 vs. Gleason 4. Such percentages are too subjective.
Fred Barone
[email protected]
Monthly Meeting: Sept 7, 2022
Speaker: Dr. Samul Karavadia (Dr. K) of Advanced Urology Institute.
Topic: Robotic Radical Prostatectomies (RRP)
Our speaker for our meeting on September 7 was Dr. Samul Karavadia (Dr. K) of Advanced Urology Institute. His talk focused upon Robotic Radical Prostatectomies (RRP).
The best way to summarize his presentation is to post two videos that he played for the audience. The first video is an animated two and a half minute presentation that is an overview of how robotic radical prostatectomy is performed.
How A RP Is Performed
The second video lasts approximately 26 minutes and shows the actual performance of an RP with the cutting and removal of tissue.
Robotic Assisted Laparoscopic Radical Prostatectomy
Robotic surgery was initiated around the year 2000. Compared to an open prostatectomy which was the standard of care at the time, it has a faster recovery, lower blood transfusion, encompasses less pain and results in better preservation of the bladder. Dr. K was trained in both open and robotic.
An RRP normally takes about 2 hours to perform, and the patient is placed under general anesthesia in a hospital setting. Dr. has had patients go home the same day as the surgery, although depending upon the patient's age, his general health profile and the severity of the cancer, a hospital stay may be required. The higher the Gleason score, the more difficult the surgery.
Certain health conditions preclude a patient from a RRP, namely blood disorders, heart conditions, prior lower abdominal surgeries (i.e. hernia where mesh is inserted) and prior radiation that obliterates the gland. He also tends to shy away from surgery if cancer is positive in the lymph nodes.
Dr. K attempts to spare the nerve bundle surrounding the prostate if possible. Based upon the MRI, it is difficult to tell where the nerves are in relation to the cancer.
Biopsies rarely cause cancer cells to spread to other areas of the body.
A question arose regarding transrectal vs. transperineal biopsies. Because a transrectal is closer to the prostate gland, Dr. K feels that a higher degree of accuracy is achieved than with a transperineal. A transrectal biopsy cannot access the anterior lobe of the prostate, however the majority of cancers are located in the posterior lobe. An MRI will show the anterior lobe and indicate if a lesion exists there. A transperineal biopsy may be appropriate in that situation.
Reference was made to a recent article indicating that a small cohort of German men, 25, had undergone RRP's without a biopsy. Prior to the surgery, the men had undergone MRI;s and PSMA pet scans. Dr. K stated that the current standard of care is an MRI and then a biopsy before any intervention. He did opine that possibly in 10 to 15 years in the future, RRP's based upon the previously mentioned scans may be the standard. More clinical trials are obviously needed.
Fred Barone
[email protected]
Speaker: Dr. Samul Karavadia (Dr. K) of Advanced Urology Institute.
Topic: Robotic Radical Prostatectomies (RRP)
Our speaker for our meeting on September 7 was Dr. Samul Karavadia (Dr. K) of Advanced Urology Institute. His talk focused upon Robotic Radical Prostatectomies (RRP).
The best way to summarize his presentation is to post two videos that he played for the audience. The first video is an animated two and a half minute presentation that is an overview of how robotic radical prostatectomy is performed.
How A RP Is Performed
The second video lasts approximately 26 minutes and shows the actual performance of an RP with the cutting and removal of tissue.
Robotic Assisted Laparoscopic Radical Prostatectomy
Robotic surgery was initiated around the year 2000. Compared to an open prostatectomy which was the standard of care at the time, it has a faster recovery, lower blood transfusion, encompasses less pain and results in better preservation of the bladder. Dr. K was trained in both open and robotic.
An RRP normally takes about 2 hours to perform, and the patient is placed under general anesthesia in a hospital setting. Dr. has had patients go home the same day as the surgery, although depending upon the patient's age, his general health profile and the severity of the cancer, a hospital stay may be required. The higher the Gleason score, the more difficult the surgery.
Certain health conditions preclude a patient from a RRP, namely blood disorders, heart conditions, prior lower abdominal surgeries (i.e. hernia where mesh is inserted) and prior radiation that obliterates the gland. He also tends to shy away from surgery if cancer is positive in the lymph nodes.
Dr. K attempts to spare the nerve bundle surrounding the prostate if possible. Based upon the MRI, it is difficult to tell where the nerves are in relation to the cancer.
Biopsies rarely cause cancer cells to spread to other areas of the body.
A question arose regarding transrectal vs. transperineal biopsies. Because a transrectal is closer to the prostate gland, Dr. K feels that a higher degree of accuracy is achieved than with a transperineal. A transrectal biopsy cannot access the anterior lobe of the prostate, however the majority of cancers are located in the posterior lobe. An MRI will show the anterior lobe and indicate if a lesion exists there. A transperineal biopsy may be appropriate in that situation.
Reference was made to a recent article indicating that a small cohort of German men, 25, had undergone RRP's without a biopsy. Prior to the surgery, the men had undergone MRI;s and PSMA pet scans. Dr. K stated that the current standard of care is an MRI and then a biopsy before any intervention. He did opine that possibly in 10 to 15 years in the future, RRP's based upon the previously mentioned scans may be the standard. More clinical trials are obviously needed.
Fred Barone
[email protected]
Monthly Meeting, July 3, 2022
Speaker: Dr. Gabe Mirkin, MD
Topic: Prostate Cancer and Health
Our speaker on August 3 was Dr. Gabe Mirkin who addressed an audience of 22 people. Dr. Mirkin is an 87-year-old health and fitness guru who bicycles in excess of 100 miles per week. During his career, he was Board Certified in four disciplines, Sports Medicine, Pediatrics, Pediatric Allergy, and Allergy and Immunology. He hosted a radio talk show for more than 20 years and currently publishes a weekly Health and Fitness Ezine. His talk focused upon lifestyle factors to help prevent and treat prostate cancer. Each slide in his presentation included an authoritative reference for the information presented. Those references are not included in this summary.
All men will develop Prostate Cancer (PCa) if they live long enough. Unlike many other cancers, prostate cancer usually grows very slowly and does not kill the vast majority of men who have it. Compared to men who do not have PCa the 15-year relative survival rate is 95%.
PCa has the same risks as diabetes and heart attacks, high blood pressure, high cholesterol and high insulin levels. Obesity increases the risk of dying from PCa by raising leptin, interleukin-6, heparin-binding epidermal growth factor like growth factor (HB-EGF), vascular endothelial growth factor (VEGF) and adiponectin.
Chemotherapy and Radiation to treat Prostate Cancer can Increase Risk for Heart Attacks. Radiation increases risk of heart failure, irregular heartbeats & heart attack'. Chemotherapy drugs damage the heart. Drugs blocking male hormones increase risk for heart attacks prostate cancer patients who use a heart-attack preventing program are far less likely to suffer recurrences.
A,B,C,D,E,F to prevent prostate cancer.
Fruits, vegetables & nuts, *soluble fiber, beans, mushrooms and seeds, onions, berries, tomatoes, tea, coffee and fish are foods that reduce the risk of PCa recurrence. Processed meats (salami, bologna, sausage, bacon and hot dogs), all meats from mammals, eggs and milk, and deep-fried foods are foods that increase the risk of PCa. Without water, sugar binds to the protein in meat to form AGEs (advanced glycation endproducts)
Nonfood risks of PCa include being overweight, a lack of exercise, alcohol, and low vitamin D.
Colon bacteria eat what you eat. HEALTHFUL BACTERIA do not try to enter your colon cells. HARMFUL BACTERIA enter colon cells to turn on your immunity to cause inflammation. Your immunity is good because it kills germs, but if it stays on all the time, it uses the same cells & chemicals to attack your genetic DNA to cause cancer. Healthful Colon Bacteria convert soluble fiber in plants to *Short Chain Fatty Acids *that increase colon mucous that *prevents harmful bacteria from penetrating colon cells *to turn on your immunity *to cause Inflammation *that increases risk for heart attacks and cancers.
Anti-inflammatory Diet Includes:
1. Unlimited vegetables, fruits, whole grains, beans, nuts & other seeds
2. Some deep-water fish
3. Poultry not associated with disease (unless skin or fried)
4. Limited refined carbohydrates (bakery products & pasta particularly if overweight or diabetic).
5. Limited sugared water, sugar-added foods.
6. Limited red meat
7. Avoidance of partially hydrogenated fats
8. Avoidance of burnt fats: Polycyclic Aromatic Hydrocarbons (PAH) and Advanced Glycation End Products (AGE)
Red meat increases the risk of diabetes and heart attacks because it decreases insulin sensitivity and Supplies Choline and lecithin that are converted to TMAO that punches holes in arteries to start plaque formation. TMAO is trimethylamine N-oxide.
A high rise in blood sugar damages every cell in one's body. Blood sugar >140 after meals damages cells. People with high blood sugar levels are at increased risk for cancers: prostate, liver, gallbladder, resp. tract, thyroid, rectum pancreas, bladder, uterus, cervix, stomach; and multiple myeloma. Refined carbohydrates cause blood sugar to rise too high. Sugar sticks to cell membranes, and once attached, never detached.
All sugar-sweetened beverages are associated with a significantly elevated risk of type 2 Diabetes Fruit juice and soft drinks increase diabetes risk by 130% Fruit: decrease diabetes risk by 80%. Fruit juices and sugared soft drinks are not stopped by the pyloric sphincter. They enter the intestines immediately to cause a rapid rise in blood sugar. An orange can stay in your stomach for 5 hours. Sugar in fruits is safe. Fruits have soluble fiber, a gel that binds to sugar in the intestines. In the colon, bacteria ferment soluble fiber to release sugar.
Whole grains prevent diabetes and do not cause a high rise in blood sugar. Grinding and cooking of whole grains raise glycemic loads. Whole grains increase insulin sensitivity, help prevent diabetes & heart attacks & lower cholesterol.
Nuts are full of fat, but not fattening. In the mouth, most almond cells remain intact after being chewed. In the upper GI tract, fat is not absorbed. In the colon, fat is released from cells by bacterial fermentation then absorbed.
Advanced Glycation End Products: Cooking without water causes sugar to attach to fat, protein, and nucleic acids to form AGEs that can damage every cell in your body. You eat them in food or form them in your body. Frying, broiling, grilling, and roasting increase AGE's while boiling, poaching, stewing, steaming and microwaving reduce AGE's.
HEART ATTACK WARNING SIGNS INCLUDEW: BP>120/80; LDL> 100; HBA1C>6; CRP>1; Abdominal obesity; Lipoprotein(a)> 125; Triglyc >150; HDL<40; Homocys>10
Almost all people with small hips and big bellies have high blood sugar levels. A fatty liver prevents liver from accepting sugar from blood.
Exercise sensitizes muscle cells to insulin to help prevent high rise in blood sugar that follows eating refined carbohydrates up to 17 hours after you finish a workout. (athletes’ recovery: maximum effect for ½ hr.)
Diets can be harmful if there is weight loss and then weight gain. The regained weight will normally rest in the liver.
Apoptosis is the death of cells which occurs as a normal and controlled part of an organisms growth. Different cells are preprogrammed to live a predetermined amount of time. Cancer is one of the scenarios where too little apoptosis occurs, resulting in malignant cells that will not die. The mechanism of apoptosis is complex and involves many pathways.
Fred Barone
[email protected]
Speaker: Dr. Gabe Mirkin, MD
Topic: Prostate Cancer and Health
Our speaker on August 3 was Dr. Gabe Mirkin who addressed an audience of 22 people. Dr. Mirkin is an 87-year-old health and fitness guru who bicycles in excess of 100 miles per week. During his career, he was Board Certified in four disciplines, Sports Medicine, Pediatrics, Pediatric Allergy, and Allergy and Immunology. He hosted a radio talk show for more than 20 years and currently publishes a weekly Health and Fitness Ezine. His talk focused upon lifestyle factors to help prevent and treat prostate cancer. Each slide in his presentation included an authoritative reference for the information presented. Those references are not included in this summary.
All men will develop Prostate Cancer (PCa) if they live long enough. Unlike many other cancers, prostate cancer usually grows very slowly and does not kill the vast majority of men who have it. Compared to men who do not have PCa the 15-year relative survival rate is 95%.
PCa has the same risks as diabetes and heart attacks, high blood pressure, high cholesterol and high insulin levels. Obesity increases the risk of dying from PCa by raising leptin, interleukin-6, heparin-binding epidermal growth factor like growth factor (HB-EGF), vascular endothelial growth factor (VEGF) and adiponectin.
Chemotherapy and Radiation to treat Prostate Cancer can Increase Risk for Heart Attacks. Radiation increases risk of heart failure, irregular heartbeats & heart attack'. Chemotherapy drugs damage the heart. Drugs blocking male hormones increase risk for heart attacks prostate cancer patients who use a heart-attack preventing program are far less likely to suffer recurrences.
A,B,C,D,E,F to prevent prostate cancer.
- Aspirin if indicated major heart attack risk
- Blood pressure monitoring
- Cholesterol management & no Cigarettes
- Diet & Diabetes Prevention: eat fruits & vegetables; restrict sugar-added foods & drinks, meat & fried foods
- Exercise
- Fat loss
Fruits, vegetables & nuts, *soluble fiber, beans, mushrooms and seeds, onions, berries, tomatoes, tea, coffee and fish are foods that reduce the risk of PCa recurrence. Processed meats (salami, bologna, sausage, bacon and hot dogs), all meats from mammals, eggs and milk, and deep-fried foods are foods that increase the risk of PCa. Without water, sugar binds to the protein in meat to form AGEs (advanced glycation endproducts)
Nonfood risks of PCa include being overweight, a lack of exercise, alcohol, and low vitamin D.
Colon bacteria eat what you eat. HEALTHFUL BACTERIA do not try to enter your colon cells. HARMFUL BACTERIA enter colon cells to turn on your immunity to cause inflammation. Your immunity is good because it kills germs, but if it stays on all the time, it uses the same cells & chemicals to attack your genetic DNA to cause cancer. Healthful Colon Bacteria convert soluble fiber in plants to *Short Chain Fatty Acids *that increase colon mucous that *prevents harmful bacteria from penetrating colon cells *to turn on your immunity *to cause Inflammation *that increases risk for heart attacks and cancers.
Anti-inflammatory Diet Includes:
1. Unlimited vegetables, fruits, whole grains, beans, nuts & other seeds
2. Some deep-water fish
3. Poultry not associated with disease (unless skin or fried)
4. Limited refined carbohydrates (bakery products & pasta particularly if overweight or diabetic).
5. Limited sugared water, sugar-added foods.
6. Limited red meat
7. Avoidance of partially hydrogenated fats
8. Avoidance of burnt fats: Polycyclic Aromatic Hydrocarbons (PAH) and Advanced Glycation End Products (AGE)
Red meat increases the risk of diabetes and heart attacks because it decreases insulin sensitivity and Supplies Choline and lecithin that are converted to TMAO that punches holes in arteries to start plaque formation. TMAO is trimethylamine N-oxide.
A high rise in blood sugar damages every cell in one's body. Blood sugar >140 after meals damages cells. People with high blood sugar levels are at increased risk for cancers: prostate, liver, gallbladder, resp. tract, thyroid, rectum pancreas, bladder, uterus, cervix, stomach; and multiple myeloma. Refined carbohydrates cause blood sugar to rise too high. Sugar sticks to cell membranes, and once attached, never detached.
All sugar-sweetened beverages are associated with a significantly elevated risk of type 2 Diabetes Fruit juice and soft drinks increase diabetes risk by 130% Fruit: decrease diabetes risk by 80%. Fruit juices and sugared soft drinks are not stopped by the pyloric sphincter. They enter the intestines immediately to cause a rapid rise in blood sugar. An orange can stay in your stomach for 5 hours. Sugar in fruits is safe. Fruits have soluble fiber, a gel that binds to sugar in the intestines. In the colon, bacteria ferment soluble fiber to release sugar.
Whole grains prevent diabetes and do not cause a high rise in blood sugar. Grinding and cooking of whole grains raise glycemic loads. Whole grains increase insulin sensitivity, help prevent diabetes & heart attacks & lower cholesterol.
Nuts are full of fat, but not fattening. In the mouth, most almond cells remain intact after being chewed. In the upper GI tract, fat is not absorbed. In the colon, fat is released from cells by bacterial fermentation then absorbed.
Advanced Glycation End Products: Cooking without water causes sugar to attach to fat, protein, and nucleic acids to form AGEs that can damage every cell in your body. You eat them in food or form them in your body. Frying, broiling, grilling, and roasting increase AGE's while boiling, poaching, stewing, steaming and microwaving reduce AGE's.
HEART ATTACK WARNING SIGNS INCLUDEW: BP>120/80; LDL> 100; HBA1C>6; CRP>1; Abdominal obesity; Lipoprotein(a)> 125; Triglyc >150; HDL<40; Homocys>10
Almost all people with small hips and big bellies have high blood sugar levels. A fatty liver prevents liver from accepting sugar from blood.
Exercise sensitizes muscle cells to insulin to help prevent high rise in blood sugar that follows eating refined carbohydrates up to 17 hours after you finish a workout. (athletes’ recovery: maximum effect for ½ hr.)
Diets can be harmful if there is weight loss and then weight gain. The regained weight will normally rest in the liver.
Apoptosis is the death of cells which occurs as a normal and controlled part of an organisms growth. Different cells are preprogrammed to live a predetermined amount of time. Cancer is one of the scenarios where too little apoptosis occurs, resulting in malignant cells that will not die. The mechanism of apoptosis is complex and involves many pathways.
Fred Barone
[email protected]
Monthly Meeting, July 3, 2022
Speaker: Dr. Maen Hussein of Florida Cancer Specialists
Topic: The Evolution of Prostate Cancer Treatments over the Last Twenty Years
On Wednesday, July 6, Dr. Maen Hussein of Florida Cancer Specialists addressed an audience of 35 people. Dr. Hussein, who has been in practice for over 20 years, is Board Certified in three disciplines, Medical Oncology, Hematology and Internal Medicine. His talk was more of a high level presentation reviewing the evolution of prostate cancer treatments over the last twenty years.
Evolution of treatment has gone from a one size fits all approach to personal care philosophy. Development of recent drugs and genomic studies of the DNA of cancer cells have led to prescribing drugs that target specific mutations. The first map of the human genome occurred in 1996. Now mapping is common.
The AR V7 gene plays a key role in the function of androgen receptors to receive testosterone, a hormone that cancer cells thrive upon. There are certain drugs that inhibit the function of the hormone receptor, apalutamide, enzalutamide and abiraterone. Studies have shown that a mutation of this gene can render these drugs ineffective. Other treatment must be employed.
Regarding PSA, speed of progression is more important than total measure. Doubling time is particularly significant. It is not abnormal for elderly men to have higher PSA readings without having cancer.
From an overall survival aspect, studies have shown that radical prostatectomies and radiation produce the same result. Side effects are different. Quality of life is important and one must choose his own best option. Many urology practices now also have a radiation practice.
Chemotherapy is not a primary choice, and only should be used when there is no other choice. It destroys all cells, not just cancer cells.
Dr. Hussein encourages second opinions. Two brains are better than one. He feels that doctors can learn from their patients.
PSMA Pet Scans are the most advanced form of imaging. They can detect cancer microorganisms that other techniques cannot. Lake Medical Imaging here in The Villages now has the ability to perform such scans.
Dr. Hussein encouraged participation in clinical trials. Florida Cancer Specialists has three clinical trial centers. Participation can change the mind of patients regarding treatment.
There is an all day Prostate Cancer Conference presented by Cancer ABC's here in The Villages scheduled for November 5. Dr. Hussein will be one of the speakers
Fred Barone
[email protected]
Speaker: Dr. Maen Hussein of Florida Cancer Specialists
Topic: The Evolution of Prostate Cancer Treatments over the Last Twenty Years
On Wednesday, July 6, Dr. Maen Hussein of Florida Cancer Specialists addressed an audience of 35 people. Dr. Hussein, who has been in practice for over 20 years, is Board Certified in three disciplines, Medical Oncology, Hematology and Internal Medicine. His talk was more of a high level presentation reviewing the evolution of prostate cancer treatments over the last twenty years.
Evolution of treatment has gone from a one size fits all approach to personal care philosophy. Development of recent drugs and genomic studies of the DNA of cancer cells have led to prescribing drugs that target specific mutations. The first map of the human genome occurred in 1996. Now mapping is common.
The AR V7 gene plays a key role in the function of androgen receptors to receive testosterone, a hormone that cancer cells thrive upon. There are certain drugs that inhibit the function of the hormone receptor, apalutamide, enzalutamide and abiraterone. Studies have shown that a mutation of this gene can render these drugs ineffective. Other treatment must be employed.
Regarding PSA, speed of progression is more important than total measure. Doubling time is particularly significant. It is not abnormal for elderly men to have higher PSA readings without having cancer.
From an overall survival aspect, studies have shown that radical prostatectomies and radiation produce the same result. Side effects are different. Quality of life is important and one must choose his own best option. Many urology practices now also have a radiation practice.
Chemotherapy is not a primary choice, and only should be used when there is no other choice. It destroys all cells, not just cancer cells.
Dr. Hussein encourages second opinions. Two brains are better than one. He feels that doctors can learn from their patients.
PSMA Pet Scans are the most advanced form of imaging. They can detect cancer microorganisms that other techniques cannot. Lake Medical Imaging here in The Villages now has the ability to perform such scans.
Dr. Hussein encouraged participation in clinical trials. Florida Cancer Specialists has three clinical trial centers. Participation can change the mind of patients regarding treatment.
There is an all day Prostate Cancer Conference presented by Cancer ABC's here in The Villages scheduled for November 5. Dr. Hussein will be one of the speakers
Fred Barone
[email protected]
Monthly Meeting, June 1st, 2022
Speaker: Wendi Demark-Wahnefried, Phd., Professor at University Alabama, Birmingham
Topic: Coping with Cancer using Amplify
Our speaker for our hybrid (Zoom and In Person) was Dr. Wendi Demark-Wahnefried, Phd, R.D. She is the Associate Director for Cancer Prevention and Control for the O'Neal Comprehensive Cancer Center at the University of Alabama Birmingham (UAB) as well as Professor and Webb Endowed Chair of Nutrition Sciences and an American Cancer Society Clinical Research Professor. Wendi is a nutrition scientist with training in biochemistry, genetics and behavioral science. She presented an overview of the diet and exercise recommendations for cancer survivors and then discussed one of the studies that she is currently conducting.
Dr. Demark-Wahnfried was kind enough to forward her slide presentation to us. I will briefly discuss key slides, however I have inserted a link below to her presentation and you can access any slides that you wish.
Diet and Exercise for Cancer Survivors
Cancer survivors are more at risk for a second incidence of cancer (1 in 5) and double the risk of dying from heart disease.
A slide of Guidelines for Diet and Exercise for Cancer Prevention and Control showed those of the World Cancer Research Fund - American Institute for Cancer Research compared to the guidelines presented by the American Cancer Society. The American Cancer Society guidelines are more stringent. Maintaining a healthy weight is the most important guideline in both studies.
A slide titled Obesity and Cancer Related Mortality reflected the increased risks of dying from cancer if obese at the time of diagnosis. The slide showed comparisons for various cancers for both men and women. If a man is obese at the time of diagnosis of Prostate Cancer (PCa), he has a 34% greater chance of dying form PCa than a man who is not obese at time of diagnosis. Liver cancer is the worst for males with greater than a 400% chance of dying from the disease.
In a meta-analysis of 18,000 men, men who gained weight after diagnosis had a 21% greater chance of biochemical recurrence and a 20% greater chance of specific mortality.
It is not necessary to achieve one's ideal body to gain healthy benefits. One slide indicated that a 3% loss of body gained health benefits. This slide also suggested self-monitoring: daily recording of weight, caloric intake and exercise regimen. Losing weight too fast can also cause loss of muscle mass. The recommendation is for two pounds per week and 1.5 pounds for people over 65
Regarding meat intake, a 3 oz. portion is equal to approximately the size of a deck of cards. This should be noted if following a guideline of 18oz red or processed meat per week.
A question arose regarding sugar. There is no research that shows that sugar causes cancer. Sugar has an impact on weight and has no nutritional value.
A meta-analysis of over 3.2 million people showed that cancer survivors who eat a healthful diet lower their risk of dying from cancer by 18% and by dying from other causes by 17%.
Dr. Demark-Wahnfried is engaged in a study for the National Cancer Institute titled "AiM Plan and Act on LIFestYles (AMPLIFY). . It is a randomized clinical trial. NCT04000880
This is a totally free diet and exercise intervention done exclusively over the internet. The intervention encompasses 48 weeks and is based upon diet and exercise recommendations of the American Institute of Cancer Research and the American Cancer Society. All necessary equipment is provided.
Participants will learn: 1) safe ways to lose weight; 2) safe ways to exercise; 3) ways to reduce exposure to pesticides; 4) information about supplements, sugar, alcohol, meat, etc. 5) tips for grocery shopping and meal preparation. Normal weekly sessions last 10 to 15 minutes of viewing with weekly challenges.
Measures are performed at baseline and every six months for up to 2 years. Measures include the following: 1) phone and computer based questionnaires to assess well-being and diet; 2) Zoom visits to assess weight/waist circumference, blood pressure, physical performance and balance: 3) muscle mass (D3 Creatine); 4) dry blood spot to test inflammatory markers; 5) activity monitors to track physical activity and sleep.
To participate in AMPLIFY, the cancer patient must be
You can obtain information about AMPLIFY at this link: AMPLIFY LINK. You can also call 833 535 7934.
Speaker: Wendi Demark-Wahnefried, Phd., Professor at University Alabama, Birmingham
Topic: Coping with Cancer using Amplify
Our speaker for our hybrid (Zoom and In Person) was Dr. Wendi Demark-Wahnefried, Phd, R.D. She is the Associate Director for Cancer Prevention and Control for the O'Neal Comprehensive Cancer Center at the University of Alabama Birmingham (UAB) as well as Professor and Webb Endowed Chair of Nutrition Sciences and an American Cancer Society Clinical Research Professor. Wendi is a nutrition scientist with training in biochemistry, genetics and behavioral science. She presented an overview of the diet and exercise recommendations for cancer survivors and then discussed one of the studies that she is currently conducting.
Dr. Demark-Wahnfried was kind enough to forward her slide presentation to us. I will briefly discuss key slides, however I have inserted a link below to her presentation and you can access any slides that you wish.
Diet and Exercise for Cancer Survivors
Cancer survivors are more at risk for a second incidence of cancer (1 in 5) and double the risk of dying from heart disease.
A slide of Guidelines for Diet and Exercise for Cancer Prevention and Control showed those of the World Cancer Research Fund - American Institute for Cancer Research compared to the guidelines presented by the American Cancer Society. The American Cancer Society guidelines are more stringent. Maintaining a healthy weight is the most important guideline in both studies.
A slide titled Obesity and Cancer Related Mortality reflected the increased risks of dying from cancer if obese at the time of diagnosis. The slide showed comparisons for various cancers for both men and women. If a man is obese at the time of diagnosis of Prostate Cancer (PCa), he has a 34% greater chance of dying form PCa than a man who is not obese at time of diagnosis. Liver cancer is the worst for males with greater than a 400% chance of dying from the disease.
In a meta-analysis of 18,000 men, men who gained weight after diagnosis had a 21% greater chance of biochemical recurrence and a 20% greater chance of specific mortality.
It is not necessary to achieve one's ideal body to gain healthy benefits. One slide indicated that a 3% loss of body gained health benefits. This slide also suggested self-monitoring: daily recording of weight, caloric intake and exercise regimen. Losing weight too fast can also cause loss of muscle mass. The recommendation is for two pounds per week and 1.5 pounds for people over 65
Regarding meat intake, a 3 oz. portion is equal to approximately the size of a deck of cards. This should be noted if following a guideline of 18oz red or processed meat per week.
A question arose regarding sugar. There is no research that shows that sugar causes cancer. Sugar has an impact on weight and has no nutritional value.
A meta-analysis of over 3.2 million people showed that cancer survivors who eat a healthful diet lower their risk of dying from cancer by 18% and by dying from other causes by 17%.
Dr. Demark-Wahnfried is engaged in a study for the National Cancer Institute titled "AiM Plan and Act on LIFestYles (AMPLIFY). . It is a randomized clinical trial. NCT04000880
This is a totally free diet and exercise intervention done exclusively over the internet. The intervention encompasses 48 weeks and is based upon diet and exercise recommendations of the American Institute of Cancer Research and the American Cancer Society. All necessary equipment is provided.
Participants will learn: 1) safe ways to lose weight; 2) safe ways to exercise; 3) ways to reduce exposure to pesticides; 4) information about supplements, sugar, alcohol, meat, etc. 5) tips for grocery shopping and meal preparation. Normal weekly sessions last 10 to 15 minutes of viewing with weekly challenges.
Measures are performed at baseline and every six months for up to 2 years. Measures include the following: 1) phone and computer based questionnaires to assess well-being and diet; 2) Zoom visits to assess weight/waist circumference, blood pressure, physical performance and balance: 3) muscle mass (D3 Creatine); 4) dry blood spot to test inflammatory markers; 5) activity monitors to track physical activity and sleep.
To participate in AMPLIFY, the cancer patient must be
- over 50 years of age
- completing primary treatment for the following cancers: localized brest, prostate, colorectum, endometrium, thyroid, kidney, and ovary; multiple myeloma and non-hodgkin's lymphomas
- overweight/obese (BMI between 25 and 50)
- moderate to strenuous physical activity.
- not enrolled in a diet or exercise program
- English speaking and an 8th grade education.
You can obtain information about AMPLIFY at this link: AMPLIFY LINK. You can also call 833 535 7934.
Monthly Meeting, May 4th, 2022
Speaker: Gabrial Delanji, PhD. Chief Scientist and Systems Director for MagForce USA
Topic: Prostate Cancer Focal Therapy with NanoTherm
Our speaker for our Zoom meeting on May 4 was Gabrial Delanji, PhD. Gabriel is a physicist and the Chief Scientist and Systems Director for MagForce USA, the US operation of a publicly held German company devoted to cancer cures. The USA arm is currently conducting a clinical trial for a prostate cancer focal therapy called NanoTherm.
NanoTherm® is an investigational treatment that uses magnetic nanoparticles and an alternating magnetic field to create heat and local ablation of the cancer lesion. Very very small iron oxide particles that have a special coating allowing them to remain suspended in water are loaded into a syringe and injected into the tumor in the prostate. A core forms in the tumor that responds to an alternating current magnet field by generating heat and killing cancer cells. The particles are injected through the perineum. An MRI defines the tumor target.
After injection of the particles, patients are then placed into an activator which generates that magnetic field. The activator is somewhat similar to a CT or MRI scanner, but unlike those scans, only the patient's middle chest to the mid thigh is under the hood of the activator. The magnet flips its north and south polarity approximately 50,000 times per second. This is different from MRI polarity that remains constant. The patient must lay on his back for an hour for the treatment. It is impossible for the patient not to move some degree during this time, at least by normal breathing. The heat source is the core of particles within the tumor and the heat source will not move. The patient can move up to eight and one half inches without hindering the integrity of the procedure.
Typically a urologist will deliver this treatment.
Before a patient undergoes the treatment, he must undergo a tolerance test. The patient enters the activator prior to any injection of particles to determine if he has any problems. Normally there is no pain associated with this procedure. At times there is heating of the skin, but not enough to cause burning. Also, the patient is awake during the procedure and can alert the technicians of any problems. The highest heat point is on the surface of the skin, not internally.
The stage 1 trial has been completed. This was a treat and reset trial. The participants received no medical benefits and had prostatectomies 3 months after the trial. Analysis of the removed prostate showed that the NanoTherm treatment was effective. The stage 1 trail was for men with advanced disease whereas the current trial is for intermediate risk patients with only one lesion. The intent is for patients who have to decide to do some sort of treatment to perform Nano Therm and delay or avoid surgery or radiation altogether.
Presently there are three activators in the U.S., San Antonio, Seattle and Sarasota.
This procedure is done in an outpatient setting and currently encompasses two days with the objective of a one day treatment in the future. . Particle injection occurs on the first day and the activator portion occurs on the second day.
Four months after the trial, there is a follow up biopsy to determine if the procedure worked. There is also a long term follow whereby participants would undergo another biopsy and a special type of pet scan.
Potentially this procedure could be used for salvage therapy, but the protocol for the current trial prohibits this.
The particles remain in the patient after the procedure. This does not preclude surgery or radiation at some future point.
For the people that have had the procedure in stage 1, there have been no immediate side effects. However, they all had their prostates removed so there is no way to isolate any side effects that would occur from the Nano Therm procedure.
If a patient receives this procedure and subsequently a second tumor appears in another part of the prostate, Nano Therm therapy can treat that lesion. For the current clinical trial, the protocol does not provide for this. The object for the commercial process is for treatment of multiple lesions either at the same time or different time.
Metallic implants below the neck are an exclusion for the current study. If one has had a hip replacement, most likely metallic implants are present.
In the labs in Germany, the Company is working on a procedure to deliver the particles to a PSMA target.
The Company has an approved product in Europe for the treatment of glioblastoma, an aggressive brain tumor. Gabriel presented a brief description of that procedure.
WEBSITES:
The website for the study her in the U.S. is:
Magforce Study
The website for the European Company:
MagForce Website
NOTE: If this site pops up with German language, there is a link on the upper right corner to switch to English.
The target for final approval for this procedure is the early part of 2023.
Fred Barone
[email protected]
407 256 0274
Speaker: Gabrial Delanji, PhD. Chief Scientist and Systems Director for MagForce USA
Topic: Prostate Cancer Focal Therapy with NanoTherm
Our speaker for our Zoom meeting on May 4 was Gabrial Delanji, PhD. Gabriel is a physicist and the Chief Scientist and Systems Director for MagForce USA, the US operation of a publicly held German company devoted to cancer cures. The USA arm is currently conducting a clinical trial for a prostate cancer focal therapy called NanoTherm.
NanoTherm® is an investigational treatment that uses magnetic nanoparticles and an alternating magnetic field to create heat and local ablation of the cancer lesion. Very very small iron oxide particles that have a special coating allowing them to remain suspended in water are loaded into a syringe and injected into the tumor in the prostate. A core forms in the tumor that responds to an alternating current magnet field by generating heat and killing cancer cells. The particles are injected through the perineum. An MRI defines the tumor target.
After injection of the particles, patients are then placed into an activator which generates that magnetic field. The activator is somewhat similar to a CT or MRI scanner, but unlike those scans, only the patient's middle chest to the mid thigh is under the hood of the activator. The magnet flips its north and south polarity approximately 50,000 times per second. This is different from MRI polarity that remains constant. The patient must lay on his back for an hour for the treatment. It is impossible for the patient not to move some degree during this time, at least by normal breathing. The heat source is the core of particles within the tumor and the heat source will not move. The patient can move up to eight and one half inches without hindering the integrity of the procedure.
Typically a urologist will deliver this treatment.
Before a patient undergoes the treatment, he must undergo a tolerance test. The patient enters the activator prior to any injection of particles to determine if he has any problems. Normally there is no pain associated with this procedure. At times there is heating of the skin, but not enough to cause burning. Also, the patient is awake during the procedure and can alert the technicians of any problems. The highest heat point is on the surface of the skin, not internally.
The stage 1 trial has been completed. This was a treat and reset trial. The participants received no medical benefits and had prostatectomies 3 months after the trial. Analysis of the removed prostate showed that the NanoTherm treatment was effective. The stage 1 trail was for men with advanced disease whereas the current trial is for intermediate risk patients with only one lesion. The intent is for patients who have to decide to do some sort of treatment to perform Nano Therm and delay or avoid surgery or radiation altogether.
Presently there are three activators in the U.S., San Antonio, Seattle and Sarasota.
This procedure is done in an outpatient setting and currently encompasses two days with the objective of a one day treatment in the future. . Particle injection occurs on the first day and the activator portion occurs on the second day.
Four months after the trial, there is a follow up biopsy to determine if the procedure worked. There is also a long term follow whereby participants would undergo another biopsy and a special type of pet scan.
Potentially this procedure could be used for salvage therapy, but the protocol for the current trial prohibits this.
The particles remain in the patient after the procedure. This does not preclude surgery or radiation at some future point.
For the people that have had the procedure in stage 1, there have been no immediate side effects. However, they all had their prostates removed so there is no way to isolate any side effects that would occur from the Nano Therm procedure.
If a patient receives this procedure and subsequently a second tumor appears in another part of the prostate, Nano Therm therapy can treat that lesion. For the current clinical trial, the protocol does not provide for this. The object for the commercial process is for treatment of multiple lesions either at the same time or different time.
Metallic implants below the neck are an exclusion for the current study. If one has had a hip replacement, most likely metallic implants are present.
In the labs in Germany, the Company is working on a procedure to deliver the particles to a PSMA target.
The Company has an approved product in Europe for the treatment of glioblastoma, an aggressive brain tumor. Gabriel presented a brief description of that procedure.
WEBSITES:
The website for the study her in the U.S. is:
Magforce Study
The website for the European Company:
MagForce Website
NOTE: If this site pops up with German language, there is a link on the upper right corner to switch to English.
The target for final approval for this procedure is the early part of 2023.
Fred Barone
[email protected]
407 256 0274
Monthly Meeting, April 6th, 2022
Speaker: Bradlee Robert, FACHE, MHA, RT. Director of Operations of the UF Health Proton Therapy Institute in Jacksonville, FL
Topic: Proton Radiation in the Treatment of PCa.
Our speaker for our meeting on Wednesday, April 6, was Bradlee Robert, FACHE, MHA, RT. Mr. Robert began his career as a radiation technologist and is now the Director of Operations of the UF Health Proton Therapy Institute in Jacksonville, FL. His talk focused on the use of proton radiation in the treatment of PCa. Twenty-five people attended this meeting.
A proton is a small particle with a positive charge within the nucleus of an atom. Proton radiation is a form of radiation treatment used to destroy tumor cells. Instead of using x-rays (photons) like regular radiation treatment, it uses protons to send beams of high energy that can target tumors. Cyclotrons accelerate the protons to two thirds the speed of light.
There are 40 proton radiation treatment centers in the United States, including two in Florida, the one in Jacksonville that Bradlee is affiliated with and one in Orlando. Both are part of the UF Healthcare system. The one in Jacksonville has 5 treatment rooms and the one in Orlando has one room. The Jacksonville facility treated its ten thousandth patient this past February.
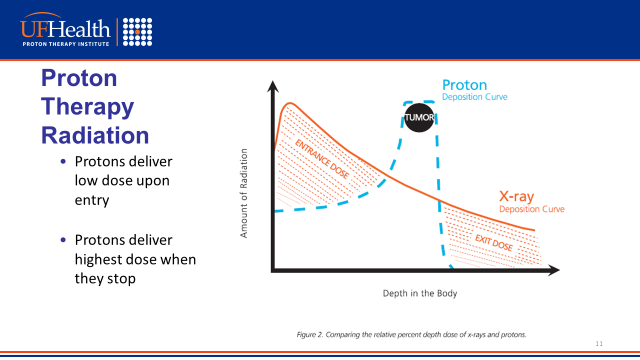
Both proton and X-ray radiation are external therapies as opposed to internal radiation, brachytherapy, where radioactive seeds are implanted into the prostate. Proton radiation stops at the target whereby X-ray does not stop in the body and exits the other side of entry
The following graph demonstrates the disposition curves of proton vs. X-ray radiation. X-ray delivers the highest dose when it enters the body while proton delivers the highest dose when it hits the target tumor.
Speaker: Bradlee Robert, FACHE, MHA, RT. Director of Operations of the UF Health Proton Therapy Institute in Jacksonville, FL
Topic: Proton Radiation in the Treatment of PCa.
Our speaker for our meeting on Wednesday, April 6, was Bradlee Robert, FACHE, MHA, RT. Mr. Robert began his career as a radiation technologist and is now the Director of Operations of the UF Health Proton Therapy Institute in Jacksonville, FL. His talk focused on the use of proton radiation in the treatment of PCa. Twenty-five people attended this meeting.
A proton is a small particle with a positive charge within the nucleus of an atom. Proton radiation is a form of radiation treatment used to destroy tumor cells. Instead of using x-rays (photons) like regular radiation treatment, it uses protons to send beams of high energy that can target tumors. Cyclotrons accelerate the protons to two thirds the speed of light.
There are 40 proton radiation treatment centers in the United States, including two in Florida, the one in Jacksonville that Bradlee is affiliated with and one in Orlando. Both are part of the UF Healthcare system. The one in Jacksonville has 5 treatment rooms and the one in Orlando has one room. The Jacksonville facility treated its ten thousandth patient this past February.
Both proton and X-ray radiation are external therapies as opposed to internal radiation, brachytherapy, where radioactive seeds are implanted into the prostate. Proton radiation stops at the target whereby X-ray does not stop in the body and exits the other side of entry
The following graph demonstrates the disposition curves of proton vs. X-ray radiation. X-ray delivers the highest dose when it enters the body while proton delivers the highest dose when it hits the target tumor.
Mr. Robert presented several slides showing both frontal and side views of the pelvic area which demonstrated the radiation flow comparing proton and X-ray radiation.
Normally the patient is in the treatment room between fifteen and twenty minutes. Of this, approximately one minute is actual radiation while the rest involve procedures to ensure an accurate treatment. Even though radiation targets a tumor or tumors, the treatment is considered whole gland because the entire prostate is affected. A normal treatment regimen consists of 39 visits but the dosage can be increased 50% reducing the visits to 28 depending upon circumstances. Proton therapy has not developed the ultra hypofractionated five regimen treatment.
Proton therapy does not have any age restrictions as opposed to certain surgeries.
Prostate size does not hinder proton radiation whereas hormone therapy is required to reduce the prostate size to an acceptable level for X-ray radiation.
Proton radiation therapy is covered by Medicare. Certain Medicare advantage plans will initially deny proton therapy because of cost. The UF center has a department that deals with this issue and has been successful in gaining approval. A member of the audience who has insurance with The Village Advantage Plan was initially denied the procedure, but he had UF intercede and coverage was approved.
A question was posed asking, which is better, radiation or surgery. Mr. Robert did not express an opinion but stated many issues affect one's decision, the aggressive of one's cancer, one's overall health condition, one's psyche among other considerations. A member of the audience stated that he went to Johns Hopkins in Baltimore for a consultation. He spent the morning meeting with individual doctors from the various types of treatments for PCa. The afternoon meeting consisted of a panel discussion with the five providers from the morning session. All expressed their opinions which did not result in a consensus agreement. The participant chose proton radiation therapy after the meeting. This service cost is about $2,500.
Fred Barone
[email protected]
Normally the patient is in the treatment room between fifteen and twenty minutes. Of this, approximately one minute is actual radiation while the rest involve procedures to ensure an accurate treatment. Even though radiation targets a tumor or tumors, the treatment is considered whole gland because the entire prostate is affected. A normal treatment regimen consists of 39 visits but the dosage can be increased 50% reducing the visits to 28 depending upon circumstances. Proton therapy has not developed the ultra hypofractionated five regimen treatment.
Proton therapy does not have any age restrictions as opposed to certain surgeries.
Prostate size does not hinder proton radiation whereas hormone therapy is required to reduce the prostate size to an acceptable level for X-ray radiation.
Proton radiation therapy is covered by Medicare. Certain Medicare advantage plans will initially deny proton therapy because of cost. The UF center has a department that deals with this issue and has been successful in gaining approval. A member of the audience who has insurance with The Village Advantage Plan was initially denied the procedure, but he had UF intercede and coverage was approved.
A question was posed asking, which is better, radiation or surgery. Mr. Robert did not express an opinion but stated many issues affect one's decision, the aggressive of one's cancer, one's overall health condition, one's psyche among other considerations. A member of the audience stated that he went to Johns Hopkins in Baltimore for a consultation. He spent the morning meeting with individual doctors from the various types of treatments for PCa. The afternoon meeting consisted of a panel discussion with the five providers from the morning session. All expressed their opinions which did not result in a consensus agreement. The participant chose proton radiation therapy after the meeting. This service cost is about $2,500.
Fred Barone
[email protected]
Monthly Meeting, March 2nd, 2022
Speaker: Dr. Debra Freeman, MD, Board Certified Radiation Oncologist, Cyberknife Centers of Tampa Bay.
Topic: Prostate Cancer Treatment using CyberKnife
Our speaker for our meeting on Wednesday, March 2, was Dr. Debra Freeman, board certified Radiation Oncologist. Dr. Freeman is affiliated with CyberKnife Centers of Tampa Bay. In 2004, Dr. Freeman and her physicist associate introduced CyberKnife radiosurgery in Naples, only the second such site in Florida. They developed the first community-based prostate radiosurgery program in the U.S. and gained national recognition as “leaders in the field. In 2008, Dr. Freeman joined the WellSpring team at CyberKnife Centers of Tampa Bay and continues to develop and promote this new technology. Participants totaled 26, with some joining on Zoom and some viewing in an in-person audience.
Definition: CyberKnife System (CK), is a robotic radiation system. The mechanical device is manufactured by Accuray Corporation. It is designed for robotic radiosurgery (SRS) and stereotactic body radiotherapy (SBRT). The CyberKnife System advertises that it has the proven ability to SRS and SBRT treatments while automatically adapting treatment delivery to motion by synchronizing with it. Radiosurgery is surgery using radiation, that is, the destruction of precisely selected areas of tissue using ionizing radiation rather than excision with a blade.
Dr. Freeman presented a 2.5-minute video demonstrating how the CK System works. You can access that video here:
You Tube CK Video
Dr. Freeman stated that the video was a promotion for Acuray but presented it to show how the system works.
The two unique differences between radiosurgery and conventional radiation therapy are 1) that the treatments are given in a much shorter period of time, four or five treatments as opposed to 45 and 2) the dosage per treatment is noticeably higher. Terminology: hypofractionated treatment vs conventionally fractionated treatment. With a slow growing cancer that PCa is in many cases, hypofractionated may have a biological advantage. Certainly, there is a convenience advantage. Hypofractionated treatments deliver radiation in a more concentrated dose fashion and in a more concentrated focus area.
CK has some unique abilities that some of the other hypofractionated devices do not. It is the only robotic system giving freedom and flexibility to move around the patient in a three-dimensional fashion. Dr. Freeman then opened the meeting to answering questions.
Q: With eight out of 12 cores positive, is CK still appropriate since you state that it is a concentrated delivery? A: CK treats the entire prostate gland. Unlike focal ablation, CK does not limit radiation to certain areas of the prostate. PCa is still a whole gland disease and will be until the medical community has tools that accurately tell practitioners where the cancer is and is not. Eight out of twelve is not a contraindication to radiosurgery because the whole gland will be treated.
Q. Is CK appropriate for patients with perineural invasion (PNI)? The presence of PNI means that the pathologist saw nerves infiltrated with cancer cells either in the biopsy specimens or later on, in the surgical specimen after a radical prostatectomy. Focal PNI is not a contraindication to radiosurgery.
Q. Would you supplement radiation with other treatments such as ADT? PNI is not necessarily an indication for ADT. It may indicate a more aggressive cancer and there may be additional evaluations that one's urologist may do to assess the aggressiveness of one's tumor. By itself it is not a contraindication of radiosurgery, and it is not by itself an indicator of ADT.
Q. Do you use SpaceOar? Yes. This is a hydro gel that is placed between the prostate and the rectum. It is used for patients receiving all types of radiation, not just CK. It is creating a space that is not naturally there. It creates a space between where the dose is delivered and the rectum.
Q, Is there a maximum prostate volume to be eligible for SBRT? There used to be a max line of 70 cc's. It is not prostate size that is a restriction but whether the treatment can meet normal dose constraints. Dr. Freeman has treated prostates as large as 120 cc's.
Q. Is any radiation given via the rectum or is it all external as shown in the video? There is no radiation given via the rectum. All radiation is external.
Q. Is radiosurgery appropriate treatment after proton radiation therapy in the event of recurrence? It can be used with caution depending on the dosage of the original treatment. In these cases, radiosurgery does not treat the entire gland but just a portion of the gland.
Q. Is the total dosage the same as the dosage with conventional 45-day radiation treatment? The number entered on the prescription paper for radiosurgery will be less than the number of Grays (Gy) on the prescription paper for standard fractionated radiation. The dosage used in radiosurgery will have a more biological effect on cancerous tissue than giving radiation in a more protracted fashion. There is a calculation called Biologically Equivalent Dose. Although the prescribed dose is not the same, the end result is that the dosage is biologically equivalent.
Q. Does that mean the side effects are mathematically the same also? Side effects are determined by what tissue gets exposed to radiation. The prostate will be affected because it will receive the majority of the radiation. If surrounding tissue (seminal vesicles, bladder, rectum) is exposed, different side effects will occur depending upon what is exposed. Because of the concentration of radiosurgery to the prostate, the effect to the surrounding tissue will be less, but there will be more early onset side effects to the functions of the prostate. The primary function of the prostate is production of seminal fluid, and after treatment there will be a change in the consistency of ejaculate. Since the prostate is radiated, and the urethra passes through the prostate, urinary side effects are probably the most common. The prostate is targeted, and it swells and becomes inflamed. Since the urethra passes through the prostate it too becomes inflamed which can result in urgency, frequency, burning Symptoms start four to five days after treatment and lasts approximately two weeks. Little chance of rectal and bladder issues and minor erectile issues because of the concentration upon the prostate.
Q. How is the precise target of radiation determined? CK uses real time imaging with X-ray imagers. Little gold, non-radioactive transducers are placed into the prostate that can be seen on the X-ray imagers. This allows for the adjustment of treatment to movement, both day to day and while treatment is ongoing. CK uses X-rays. Other devices used in radiosurgery are linear accelerators that use CT scans and a newer device that is a MRI based system. These also allow for the adjustment to movement.
Q. If there is suspicion of PCa recurrence after treatment because of a rising PSA but a negative Gallium 68 scan, can radiosurgery be used for treatment? Radiosurgery needs a target. If no target can be identified on a scan, then conventional radiation would be appropriate.
Q. Where in the area of The Villages can someone receive CK treatment?
There is a CK treatment center in Gainesville and Dr. Freeman's center in Tampa.
Q. Given the low risk of a 3+3 Gleason metastasizing, does Dr. Freeman recommend CK? To make a decision to have treatment of any kind with a 3+3 Gleason is a discussion to have with a patient's team of doctors. All 3+3 Gleasons are not the same. Genetic profiles, general overall health, age, comorbidity, and the patient's desires all affect the decision. Dr. Freeman has treated patients with 3+3 but also has recommended active surveillance for other 3+3 patients. Each case is different.
Q. Is CK covered by Medicare? Medicare covers radiosurgery with CK one of the tools of radiosurgery.
Q. An attendee stated that his urologist stated that robotic surgery has made significant advances in recent years and advised him to avoid CK because there is not enough data available about the method. A. Dr. stated that in 2005 that was the case, but now there is 15 years’ worth of data. She offered to send the urologist available data.
A comment was made by one of the attendees that he had SBRT in Lady Lake. The person had SBRT but not CK.
Q. What options are available if there is a cancer recurrence after CK? A. The options depend upon where the cancer occurs. If the cancer occurs in the prostate, the options are surgery, re-radiation, cryotherapy, or laser ablation. Sometimes repeat CK. If the recurrence is outside the prostate, the treatment must be tailored to where the recurrence is.
Q. Is genomic testing appropriate for AS? A. Dr. is not talking about genomic testing to determine the risk of PCa but in the context of obtaining a more detailed molecular analysis for someone who has already been diagnosed with PCa to help determine potential aggressiveness. Yes it is appropriate and she mentioned Decipher Scores and Prolaris Scores. She uses these scores to determine which patients might be better suited for treatment rather than AS. The scores can be obtained as long as the biopsy samples are available. These tests are not routine but are becoming more utilized. The tests can be requested by the patient and they are covered by insurance.
Q. How long does an individual CK treatment last? A. A CK treatment takes about thirty to thirty-five minutes because of the movement of the machine adjusting to various angles of delivery. Other radiosurgery devices typically take less than five minutes. After the meeting, I got a follow up question from an individual who previously had proton radiation therapy. He was required to have a full bladder and stated that thirty-five minutes would be very difficult to maintain a full bladder. I corresponded with Dr. Freeman and got this response: . We do not require a full bladder for CyberKnife treatment; only partially full. In addition, if a patient needs to urinate during the 30-40 min treatment, we can allow him to get up from the table, urinate, then resume treatment where we left off.
Fred Barone
[email protected]
Speaker: Dr. Debra Freeman, MD, Board Certified Radiation Oncologist, Cyberknife Centers of Tampa Bay.
Topic: Prostate Cancer Treatment using CyberKnife
Our speaker for our meeting on Wednesday, March 2, was Dr. Debra Freeman, board certified Radiation Oncologist. Dr. Freeman is affiliated with CyberKnife Centers of Tampa Bay. In 2004, Dr. Freeman and her physicist associate introduced CyberKnife radiosurgery in Naples, only the second such site in Florida. They developed the first community-based prostate radiosurgery program in the U.S. and gained national recognition as “leaders in the field. In 2008, Dr. Freeman joined the WellSpring team at CyberKnife Centers of Tampa Bay and continues to develop and promote this new technology. Participants totaled 26, with some joining on Zoom and some viewing in an in-person audience.
Definition: CyberKnife System (CK), is a robotic radiation system. The mechanical device is manufactured by Accuray Corporation. It is designed for robotic radiosurgery (SRS) and stereotactic body radiotherapy (SBRT). The CyberKnife System advertises that it has the proven ability to SRS and SBRT treatments while automatically adapting treatment delivery to motion by synchronizing with it. Radiosurgery is surgery using radiation, that is, the destruction of precisely selected areas of tissue using ionizing radiation rather than excision with a blade.
Dr. Freeman presented a 2.5-minute video demonstrating how the CK System works. You can access that video here:
You Tube CK Video
Dr. Freeman stated that the video was a promotion for Acuray but presented it to show how the system works.
The two unique differences between radiosurgery and conventional radiation therapy are 1) that the treatments are given in a much shorter period of time, four or five treatments as opposed to 45 and 2) the dosage per treatment is noticeably higher. Terminology: hypofractionated treatment vs conventionally fractionated treatment. With a slow growing cancer that PCa is in many cases, hypofractionated may have a biological advantage. Certainly, there is a convenience advantage. Hypofractionated treatments deliver radiation in a more concentrated dose fashion and in a more concentrated focus area.
CK has some unique abilities that some of the other hypofractionated devices do not. It is the only robotic system giving freedom and flexibility to move around the patient in a three-dimensional fashion. Dr. Freeman then opened the meeting to answering questions.
Q: With eight out of 12 cores positive, is CK still appropriate since you state that it is a concentrated delivery? A: CK treats the entire prostate gland. Unlike focal ablation, CK does not limit radiation to certain areas of the prostate. PCa is still a whole gland disease and will be until the medical community has tools that accurately tell practitioners where the cancer is and is not. Eight out of twelve is not a contraindication to radiosurgery because the whole gland will be treated.
Q. Is CK appropriate for patients with perineural invasion (PNI)? The presence of PNI means that the pathologist saw nerves infiltrated with cancer cells either in the biopsy specimens or later on, in the surgical specimen after a radical prostatectomy. Focal PNI is not a contraindication to radiosurgery.
Q. Would you supplement radiation with other treatments such as ADT? PNI is not necessarily an indication for ADT. It may indicate a more aggressive cancer and there may be additional evaluations that one's urologist may do to assess the aggressiveness of one's tumor. By itself it is not a contraindication of radiosurgery, and it is not by itself an indicator of ADT.
Q. Do you use SpaceOar? Yes. This is a hydro gel that is placed between the prostate and the rectum. It is used for patients receiving all types of radiation, not just CK. It is creating a space that is not naturally there. It creates a space between where the dose is delivered and the rectum.
Q, Is there a maximum prostate volume to be eligible for SBRT? There used to be a max line of 70 cc's. It is not prostate size that is a restriction but whether the treatment can meet normal dose constraints. Dr. Freeman has treated prostates as large as 120 cc's.
Q. Is any radiation given via the rectum or is it all external as shown in the video? There is no radiation given via the rectum. All radiation is external.
Q. Is radiosurgery appropriate treatment after proton radiation therapy in the event of recurrence? It can be used with caution depending on the dosage of the original treatment. In these cases, radiosurgery does not treat the entire gland but just a portion of the gland.
Q. Is the total dosage the same as the dosage with conventional 45-day radiation treatment? The number entered on the prescription paper for radiosurgery will be less than the number of Grays (Gy) on the prescription paper for standard fractionated radiation. The dosage used in radiosurgery will have a more biological effect on cancerous tissue than giving radiation in a more protracted fashion. There is a calculation called Biologically Equivalent Dose. Although the prescribed dose is not the same, the end result is that the dosage is biologically equivalent.
Q. Does that mean the side effects are mathematically the same also? Side effects are determined by what tissue gets exposed to radiation. The prostate will be affected because it will receive the majority of the radiation. If surrounding tissue (seminal vesicles, bladder, rectum) is exposed, different side effects will occur depending upon what is exposed. Because of the concentration of radiosurgery to the prostate, the effect to the surrounding tissue will be less, but there will be more early onset side effects to the functions of the prostate. The primary function of the prostate is production of seminal fluid, and after treatment there will be a change in the consistency of ejaculate. Since the prostate is radiated, and the urethra passes through the prostate, urinary side effects are probably the most common. The prostate is targeted, and it swells and becomes inflamed. Since the urethra passes through the prostate it too becomes inflamed which can result in urgency, frequency, burning Symptoms start four to five days after treatment and lasts approximately two weeks. Little chance of rectal and bladder issues and minor erectile issues because of the concentration upon the prostate.
Q. How is the precise target of radiation determined? CK uses real time imaging with X-ray imagers. Little gold, non-radioactive transducers are placed into the prostate that can be seen on the X-ray imagers. This allows for the adjustment of treatment to movement, both day to day and while treatment is ongoing. CK uses X-rays. Other devices used in radiosurgery are linear accelerators that use CT scans and a newer device that is a MRI based system. These also allow for the adjustment to movement.
Q. If there is suspicion of PCa recurrence after treatment because of a rising PSA but a negative Gallium 68 scan, can radiosurgery be used for treatment? Radiosurgery needs a target. If no target can be identified on a scan, then conventional radiation would be appropriate.
Q. Where in the area of The Villages can someone receive CK treatment?
There is a CK treatment center in Gainesville and Dr. Freeman's center in Tampa.
Q. Given the low risk of a 3+3 Gleason metastasizing, does Dr. Freeman recommend CK? To make a decision to have treatment of any kind with a 3+3 Gleason is a discussion to have with a patient's team of doctors. All 3+3 Gleasons are not the same. Genetic profiles, general overall health, age, comorbidity, and the patient's desires all affect the decision. Dr. Freeman has treated patients with 3+3 but also has recommended active surveillance for other 3+3 patients. Each case is different.
Q. Is CK covered by Medicare? Medicare covers radiosurgery with CK one of the tools of radiosurgery.
Q. An attendee stated that his urologist stated that robotic surgery has made significant advances in recent years and advised him to avoid CK because there is not enough data available about the method. A. Dr. stated that in 2005 that was the case, but now there is 15 years’ worth of data. She offered to send the urologist available data.
A comment was made by one of the attendees that he had SBRT in Lady Lake. The person had SBRT but not CK.
Q. What options are available if there is a cancer recurrence after CK? A. The options depend upon where the cancer occurs. If the cancer occurs in the prostate, the options are surgery, re-radiation, cryotherapy, or laser ablation. Sometimes repeat CK. If the recurrence is outside the prostate, the treatment must be tailored to where the recurrence is.
Q. Is genomic testing appropriate for AS? A. Dr. is not talking about genomic testing to determine the risk of PCa but in the context of obtaining a more detailed molecular analysis for someone who has already been diagnosed with PCa to help determine potential aggressiveness. Yes it is appropriate and she mentioned Decipher Scores and Prolaris Scores. She uses these scores to determine which patients might be better suited for treatment rather than AS. The scores can be obtained as long as the biopsy samples are available. These tests are not routine but are becoming more utilized. The tests can be requested by the patient and they are covered by insurance.
Q. How long does an individual CK treatment last? A. A CK treatment takes about thirty to thirty-five minutes because of the movement of the machine adjusting to various angles of delivery. Other radiosurgery devices typically take less than five minutes. After the meeting, I got a follow up question from an individual who previously had proton radiation therapy. He was required to have a full bladder and stated that thirty-five minutes would be very difficult to maintain a full bladder. I corresponded with Dr. Freeman and got this response: . We do not require a full bladder for CyberKnife treatment; only partially full. In addition, if a patient needs to urinate during the 30-40 min treatment, we can allow him to get up from the table, urinate, then resume treatment where we left off.
Fred Barone
[email protected]
Monthly Meeting, Feb 2nd, 2022
Speaker: Jan Manarite, Executive Vice President, Cancer ABCs and Patient Advocate
Topic: Cancer Diagnosis and Treatment, Questions and Answers
Jan Manarite was our speaker via Zoom for our meeting on February 2. Twenty-Five people attended the Zoom session and 12 attended the in person audience. Jan is Executive Vice President of Cancer ABCs and an award winning advocate. She became involved as a caregiver when her husband was diagnosed at age 58 with a PSA over 7,000 and cancer that had already metastasized. He survived thirteen years. The format of the presentation was a question and answer forum.
Before she started fielding questions, she stressed the importance of obtaining and actually reading one's medical records. They will normally contain big words that are not initially understood but can easily be found by using Google. This will help a patient understand his cancer and ask better questions. .
Jan also explained she has produced 4 patient conferences, 2 in Virginia and 2 in Florida. She and Joel (Cancer ABCs) had scheduled and postponed 3 conferences here in The Villages because of the pandemic and have now scheduled one for Saturday, November 5th of this year, at The Brownwood Hotel & Spa. Save that Date! Her conference format includes a large opening session where everybody participates and then several smaller break out sessions on different topics allowing participants to choose those topics that are important to them and their PCa journeys because all cancers are different.
The first questions involved shared decision making. Basically it means that the doctor shares his decision with the patient and the patient shares his with the doctor. Do not go into meetings appointments and have the doctor make all the decisions for you. There is medical data supporting shared decision making. Normally when patients mention shared decision making, that is when the meaningful conversation with the doctor starts.
Jan was asked how her husband survived for 13 years with such a bad diagnosis. Jan feels that her husband lasted so long because they became involved in getting his records, reading the records, asking questions and being part of the decision. This is a one step at a time process and involves research and lots of questions.
A participant recently had a transperineal biopsy but the urologist took 10 samples rather than the normal 12 that appears to be the standard of care. Jan suggested that going forward to develop a list of questions and expectations including the number of cores. If the number is not acceptable to the patient, then it is not acceptable. This needs to be a conversation with the urologist, even if it takes time.
Jan then explained the difference between transrectal (TR) and transperineal biopsies (TP). There has recently been a push for TP because of the risk of infection with TR because of the presence of e coli in the rectum.
How does one get the doctor to spend the time that you require to get the answers that you need? Often a local support group can share experiences with certain providers regarding physicians who provide the needed time. It is important to develop a relationship with all of your doctors and become comfortable with them. Jan and her husband switched doctors 4 times during their 13-year journey.
A participant indicated that he is in the process of making a treatment decision. He has ruled out radical prostatectomy and is investigating Transurethral Ultrasound Ablation (Tulsa Pro). (Read more here - https://profoundmedical.com/new-tulsa/) He seemed frustrated because nothing is a guaranteed cure. Jan commented that nothing in science is perfect. No procedure is 100% guaranteed. Another participant posted that Tulsa Pro costs between $14,000 and $35,000 and it is not covered by Medicare. Jan stressed to always ask what any procedure will cost and what is or is not covered by insurance. There is not a lot of data on Tulsa Pro, compared to some other procedures, including radiation. Why choose something with little data that will cost significant dollars when there are treatments covered by insurance that have more data and research?
Jan briefly summarized the types of radiation oncology and indicated that there is good literature on CyberKnife. Jan also indicated that hormone therapy may be added to radiation to shrink the prostate if it is too large to minimize the risk of damage to surrounding tissue. Radiation oncologists can issue prescriptions for hormone therapy in pill form, now that Orgovyx is a new type of hormone therapy in pills (instead of shots). The participant in question indicated that his prostate size is 40 ccs. This should be small enough for radiation without hormone therapy to shrink the prostate. Of course, always ask your radiation oncologist.
A question arose regarding recording doctor's visits. Jan is nor aware of the legalities regarding recording surreptitiously. It is wise to take another person with you into an appointment to have another set of ears. This ability has been limited by the pandemic. It is a good idea to request permission to record a meeting if another person cannot join you in an appointment.
A participant indicated that he has recently been diagnosed with a 4,000 PSA and stage 4 cancer. He is being treated by an urologist who has prescribed hormone therapy. His PSA is now 68. Jan strongly suggested that he consult with a medical oncologist. An urologist is a surgeon. A medical oncologist is trained in internal medicine and treats all cancers and is more knowledgeable regarding side effects. Jan inquired about bone (osteoporosis) tests. The participant indicated that he has done that and has been diagnosed with osteopenia and is undergoing treatment. The participant indicated that he has a strong relationship with his urologist and Jan repeated that relationship is the most important thing.
Jan referenced an article that she wrote "Understanding Survival Statistics". Doctors may come into an appointment and say that one's PSA is such and such and that person has two or three years to live. The doctors do not know. Everyone is different and science keeps moving and developing. The three major disciplines, urology, radiology and oncology have major conferences each year where new data is presented and published leading to new treatment options. Nobody knows how long one will live.
Regarding going to a university or major cancer center as opposed to a community doctor, Jan feels that there are certain benefits. 1) They will be tapped into more clinical trials but the downside is that they may try to sell a patient a clinical trial. 2) At a university research hospital or cancer center a patient may be given a tumor board evaluation where an urologist, radiation oncologist and medical oncologist review a patient's case as a team. The patient gets a broad perspective of his case. But Jan reiterated that the relationship with the doctor is the most important thing, in her experience.
If one is looking at adding complementary medicine or alternative medicine, what is the approach in bringing it up to one's standard of care doctor? This is where relationships are important. One must make sure that he has done research on the alternative treatment and be able to answer the doctor's questions. One must discern whether the alternative treatment is not merely an attempt to sell a product or service. One must be able to explain how to measure success of the alternative treatment. It is always important to discuss the alternative treatment with the standard of care doctor because it may interfere with his treatment.
What should one look for in a doctor? Jane reiterated the importance of relationships. Find a doctor who is willing to hear your questions and answer them and allow you to participate in shared decision making. Another comment was that for whatever treatment one wants to receive, find a doctor that performs this procedure routinely and often, not one who performs the procedure occasionally. Reference was made to Dr. Vipul Patel of Advent Health who has performed over 15,000 robotic prostatectomies.
Jan was asked to comment on Proton Beam Radiation versus the other types. Jan mentioned that Proton Beam is usually the most expensive - maybe three times the cost of Cyberknife. Ask, if that is a concern for you. Cyberknife is the brand name of a type of equipment that delivers a certain type of radiation called SBRT. Each radiation treatment is called a fraction. Hypofractionated treatment means fewer number of treatments. One should ask the radiation oncologist how many treatments are required. In her knowledge with medical professionals, Jan indicated that Cyberknife/ SBRT has had very good data released over the last several years.
Read more about SBRT Here.
Jan mentioned PSMA Pet Scans. There are two different types, one is only available in California and the other, called Pylarify, is more widely available. It is currently available in Orlando and Gainesville (contact Jan for this info on Orlando or Gainesville) and will be available sometime in the future in The Villages. PSMA involves an injection and is approved for two conditions: 1) Men with prostate cancer with suspected metastasis and 2) men with suspected recurrence with elevated PSA. Insurance will not pay if a patient does fall into one of these two categories. Information regarding this Pylarify PSMA can be found at the following website:
https://www.pylarify.com/
If anyone wants to follow up with Jan, her email is [email protected]
Fred Barone
[email protected]
Speaker: Jan Manarite, Executive Vice President, Cancer ABCs and Patient Advocate
Topic: Cancer Diagnosis and Treatment, Questions and Answers
Jan Manarite was our speaker via Zoom for our meeting on February 2. Twenty-Five people attended the Zoom session and 12 attended the in person audience. Jan is Executive Vice President of Cancer ABCs and an award winning advocate. She became involved as a caregiver when her husband was diagnosed at age 58 with a PSA over 7,000 and cancer that had already metastasized. He survived thirteen years. The format of the presentation was a question and answer forum.
Before she started fielding questions, she stressed the importance of obtaining and actually reading one's medical records. They will normally contain big words that are not initially understood but can easily be found by using Google. This will help a patient understand his cancer and ask better questions. .
Jan also explained she has produced 4 patient conferences, 2 in Virginia and 2 in Florida. She and Joel (Cancer ABCs) had scheduled and postponed 3 conferences here in The Villages because of the pandemic and have now scheduled one for Saturday, November 5th of this year, at The Brownwood Hotel & Spa. Save that Date! Her conference format includes a large opening session where everybody participates and then several smaller break out sessions on different topics allowing participants to choose those topics that are important to them and their PCa journeys because all cancers are different.
The first questions involved shared decision making. Basically it means that the doctor shares his decision with the patient and the patient shares his with the doctor. Do not go into meetings appointments and have the doctor make all the decisions for you. There is medical data supporting shared decision making. Normally when patients mention shared decision making, that is when the meaningful conversation with the doctor starts.
Jan was asked how her husband survived for 13 years with such a bad diagnosis. Jan feels that her husband lasted so long because they became involved in getting his records, reading the records, asking questions and being part of the decision. This is a one step at a time process and involves research and lots of questions.
A participant recently had a transperineal biopsy but the urologist took 10 samples rather than the normal 12 that appears to be the standard of care. Jan suggested that going forward to develop a list of questions and expectations including the number of cores. If the number is not acceptable to the patient, then it is not acceptable. This needs to be a conversation with the urologist, even if it takes time.
Jan then explained the difference between transrectal (TR) and transperineal biopsies (TP). There has recently been a push for TP because of the risk of infection with TR because of the presence of e coli in the rectum.
How does one get the doctor to spend the time that you require to get the answers that you need? Often a local support group can share experiences with certain providers regarding physicians who provide the needed time. It is important to develop a relationship with all of your doctors and become comfortable with them. Jan and her husband switched doctors 4 times during their 13-year journey.
A participant indicated that he is in the process of making a treatment decision. He has ruled out radical prostatectomy and is investigating Transurethral Ultrasound Ablation (Tulsa Pro). (Read more here - https://profoundmedical.com/new-tulsa/) He seemed frustrated because nothing is a guaranteed cure. Jan commented that nothing in science is perfect. No procedure is 100% guaranteed. Another participant posted that Tulsa Pro costs between $14,000 and $35,000 and it is not covered by Medicare. Jan stressed to always ask what any procedure will cost and what is or is not covered by insurance. There is not a lot of data on Tulsa Pro, compared to some other procedures, including radiation. Why choose something with little data that will cost significant dollars when there are treatments covered by insurance that have more data and research?
Jan briefly summarized the types of radiation oncology and indicated that there is good literature on CyberKnife. Jan also indicated that hormone therapy may be added to radiation to shrink the prostate if it is too large to minimize the risk of damage to surrounding tissue. Radiation oncologists can issue prescriptions for hormone therapy in pill form, now that Orgovyx is a new type of hormone therapy in pills (instead of shots). The participant in question indicated that his prostate size is 40 ccs. This should be small enough for radiation without hormone therapy to shrink the prostate. Of course, always ask your radiation oncologist.
A question arose regarding recording doctor's visits. Jan is nor aware of the legalities regarding recording surreptitiously. It is wise to take another person with you into an appointment to have another set of ears. This ability has been limited by the pandemic. It is a good idea to request permission to record a meeting if another person cannot join you in an appointment.
A participant indicated that he has recently been diagnosed with a 4,000 PSA and stage 4 cancer. He is being treated by an urologist who has prescribed hormone therapy. His PSA is now 68. Jan strongly suggested that he consult with a medical oncologist. An urologist is a surgeon. A medical oncologist is trained in internal medicine and treats all cancers and is more knowledgeable regarding side effects. Jan inquired about bone (osteoporosis) tests. The participant indicated that he has done that and has been diagnosed with osteopenia and is undergoing treatment. The participant indicated that he has a strong relationship with his urologist and Jan repeated that relationship is the most important thing.
Jan referenced an article that she wrote "Understanding Survival Statistics". Doctors may come into an appointment and say that one's PSA is such and such and that person has two or three years to live. The doctors do not know. Everyone is different and science keeps moving and developing. The three major disciplines, urology, radiology and oncology have major conferences each year where new data is presented and published leading to new treatment options. Nobody knows how long one will live.
Regarding going to a university or major cancer center as opposed to a community doctor, Jan feels that there are certain benefits. 1) They will be tapped into more clinical trials but the downside is that they may try to sell a patient a clinical trial. 2) At a university research hospital or cancer center a patient may be given a tumor board evaluation where an urologist, radiation oncologist and medical oncologist review a patient's case as a team. The patient gets a broad perspective of his case. But Jan reiterated that the relationship with the doctor is the most important thing, in her experience.
If one is looking at adding complementary medicine or alternative medicine, what is the approach in bringing it up to one's standard of care doctor? This is where relationships are important. One must make sure that he has done research on the alternative treatment and be able to answer the doctor's questions. One must discern whether the alternative treatment is not merely an attempt to sell a product or service. One must be able to explain how to measure success of the alternative treatment. It is always important to discuss the alternative treatment with the standard of care doctor because it may interfere with his treatment.
What should one look for in a doctor? Jane reiterated the importance of relationships. Find a doctor who is willing to hear your questions and answer them and allow you to participate in shared decision making. Another comment was that for whatever treatment one wants to receive, find a doctor that performs this procedure routinely and often, not one who performs the procedure occasionally. Reference was made to Dr. Vipul Patel of Advent Health who has performed over 15,000 robotic prostatectomies.
Jan was asked to comment on Proton Beam Radiation versus the other types. Jan mentioned that Proton Beam is usually the most expensive - maybe three times the cost of Cyberknife. Ask, if that is a concern for you. Cyberknife is the brand name of a type of equipment that delivers a certain type of radiation called SBRT. Each radiation treatment is called a fraction. Hypofractionated treatment means fewer number of treatments. One should ask the radiation oncologist how many treatments are required. In her knowledge with medical professionals, Jan indicated that Cyberknife/ SBRT has had very good data released over the last several years.
Read more about SBRT Here.
Jan mentioned PSMA Pet Scans. There are two different types, one is only available in California and the other, called Pylarify, is more widely available. It is currently available in Orlando and Gainesville (contact Jan for this info on Orlando or Gainesville) and will be available sometime in the future in The Villages. PSMA involves an injection and is approved for two conditions: 1) Men with prostate cancer with suspected metastasis and 2) men with suspected recurrence with elevated PSA. Insurance will not pay if a patient does fall into one of these two categories. Information regarding this Pylarify PSMA can be found at the following website:
https://www.pylarify.com/
If anyone wants to follow up with Jan, her email is [email protected]
Fred Barone
[email protected]
Monthly Meeting, Jan 5th, 2022
Speaker: April Rosso, MS, RDN, CSO, LD/R, Florida Cancer Specialists and Research Institute
Topic: Cancer Prevention and Cancer Recurrence
Our speaker for our meeting on January 5th was April Rosso, MS, RDN, CSO, LD/R. She is the Clinical Oncologist Dietitian Lead for Region III for Florida Cancer Specialists and Research Institute. Her presentation was delivered via Zoom to an in-person audience of 35 with an additional 14 participants attending virtually. Her talk focused upon the American Institute of Cancer Research (AICR) and their recommendations for cancer prevention and cancer recurrence. The recommendations come from a continuous research project in collaboration with the World Cancer Research Fund.
Weight and Activity
[email protected]
Speaker: April Rosso, MS, RDN, CSO, LD/R, Florida Cancer Specialists and Research Institute
Topic: Cancer Prevention and Cancer Recurrence
Our speaker for our meeting on January 5th was April Rosso, MS, RDN, CSO, LD/R. She is the Clinical Oncologist Dietitian Lead for Region III for Florida Cancer Specialists and Research Institute. Her presentation was delivered via Zoom to an in-person audience of 35 with an additional 14 participants attending virtually. Her talk focused upon the American Institute of Cancer Research (AICR) and their recommendations for cancer prevention and cancer recurrence. The recommendations come from a continuous research project in collaboration with the World Cancer Research Fund.
Weight and Activity
- Be a healthy weight and be physically active. Overweight and obesity increases the risk of 12 different types of cancer. Physical activity can lower the risk of prostate cancer and promote a healthy weight. Start slowly and work up to 30 minutes per day, 5 days of week.
- Physical activity does not have to be boot camp exercise. Chores, short walks,weight bearing walks, dancing. Make it fun. Joining a group provides support.
- Eat a plant based diet. Eat a larger portion of whole grains, vegetables, fruits, legumes, nuts and seeds and a smaller portion of animal protein: red meat, chicken, seafood, eggs.
- The New American Plate espoused the idea that at least two thirds of the plate is plant based.
- Five servings a day of fruits and vegetables. 1/2 cup cooked or 1 cup raw = 1 serving. One banana is normally considered two servings. A giant salad is two or three servings of vegetables. Not difficult to get 5 servings.
- The more the color the better. Different colors bring different nutrients.
- Use both raw and cooked fruits and vegetables.
- Calciferous vegetables (broccoli, cauliflower, cabbage, brussel sprouts). Research has shown that these vegetables may reduce cancer risk. Mix fruits and vegetables into breakfast, snacks and desserts. Add fruits to yogurt and veggies to eggs.
- For sweet tooth, eat fruit for dessert. Jazz it up with a little bit of peanut butter and cinnamon or melted chocolate chips.
- Make at least 50% of carbs whole grain, brown rice, whole wheat bread, quinoa, barley, bulgur wheat. These grains can be used in soups, stews and casseroles. Steel cut oatmeal and popcorn (not microwave popcorn smothered in butter) are also grains.
- Goal is 30 grams per day of fiber. Fiber in diet is good for gut health, helps keep things regular and helps reduce the risk of colon cancer. Build up slowly to 30 grams.
- Limit red meat, beef, pork, lamb to 18 ounces per week. More than 18 ounces per week is linked with a higher occurrence of cancer.
- Eat little if any processed meats (hot dogs, ham, deli, meat, bacon, sausage, pepperoni, salami). These contain preservatives, nitrates and nitrites, which have shown to be carcinogenic. There are certain luncheon meats made without nitrates or nitrites. Package will say "Free of nitrates and nitrites'.
- For those who are big fans of sandwiches think of chicken salad, veggies with hummus, peanut butter and banana, and cooked chicken or turkey sliced.
- Meatless meals could include beans and rice, meatless burritos or tacos, tofu or tempeh.
- Decrease the meat in casseroles and soups and add extra vegetables or beans, or use chicken or turkey instead.
- Mixed research regarding harmful effects. Use in moderation or eliminate completely.
- Diary is the main source of calcium. ADT (luporn, elegard, etc.) increases the risk of bone loss. Men on ADT need to make sure they get enough calcium in their diets.
- 4 or more servings per day increase the risk of prostate cancer. 1 cup of milk, 1.5 oz. cheese, or 1 cup of yogurt equal 1 serving. Low fat or nonfat milk is recommended if dairy is in one's diet. Dairy alternatives, (almond milk, soy milk, coconut milk) are usually fortified and provide sources of calcium.
- It is carcinogenic. Some studies have shown that even in moderate amounts, intake increases the risk of cancer. The jury is still out on how much is safe. Current recommendation is 1 drink per day for women and 2 drinks for men. This has not been changed up to this point, but some studies have shown that even this amount can increase cancer risk.
- Ground flax seeds. They can be put in oatmeal, salad dressings, and yogurt. They are a good source of phytoestrogens which are also in soy. Studies are unclear on the relationship of Phytoestrogens and prostate cancer. Some studies have shown a protective effect. Many asian countries with diets rich in phytoestrogens have lower rates of hormone related cancers. This is not a proven cause and effect.
- Some studies have shown that ground flax seed in the diet may reduce the level of PSA and slow tumor growth.
- Do not use flax seed oil. There are no phytoestrogens, only fat, and that may increase cancer risk.
- Research has not shown that supplements lower the risk of prostate cancer. Some supplements like Vitamin E may actually increase the risk of prostate cancer. A healthy diet has been shown to be more beneficial than taking supplements.
- Talk to your doctor if you are interested in certain supplements and make sure they are not contr-indicated with conditions and prescriptions.
- American Institute for Cancer Research: https://www.aicr.org/
- National Cancer Institute https://www.cancer.gov/
- USDA My Plate https://www.choosemyplate.gov
- Activia yogurt at one per day is a good choice. Greek yogurts are better because they are higher in proteins. The Fage brand is her favorite. It is lower in sugar.
- Chickpea pasta is a good source of protein. By itself, the taste may be difficult
- Processed meats are a Class I carcinogenic per the WHO because of the nitrates and nitrites.
- April had no suggestions for supplements for BPH.
- A teaspoon or half of a teaspoon of honey in tea is perfectly fine. April puts a small amount of honey in her Greek yogurt. This is a lot less sugar than what the flavored yogurts contain. Problem with sugar is not that a small amount in the diet causes cancer. The problem is that large amounts cause excess calories, weight gain and diabetes. Those things are linked with increased cancer risk.
- April has a mixed opinion on plant based meats which are now plentiful on the market. It is plant based allowing one to get plants into one's diet and enjoy the taste of red meat. The bad news is that these are processed foods and contain excess salt and the extra ingredients that are not healthy. She feels that these should not be the go to for the everyday meatless meal.
- Farm raised vs. wild caught fish is more of an ethical discussion than a nutritional discussion. Farm raised may contain a higher fat content.
- April has not advised against eating eggs for people with prostate cancer. The comment from the audience member was that egg yolks contain choline which augments prostate cancer. April has not seen anything in the research on this issue.
- Chicken, fish and red meat in limited quantities can be sources of B-12 as opposed to supplements. If B-12 deficient, supplements have a place.
- Nutritional studies result in correlations rather than cause and effect fact. That is why labels say "may cause or possibly may cause" rather than saying "does cause".
- Smoothies are good in that they allow you to get extra servings of fruits and vegetables in one meal. April does not recommend commercial establishment smoothies because they are loaded with tons of calories and sugars. Protein powder can be added.
- Wild game has less fat and cholesterol than farm raised meat. No difference regarding other nutrients.
- Nuts are fantastic. They are plants, and are a great source of protein and heart healthy fats. They are high in calories. 1/4 cup is a serving.
- For oatmeal, April suggests steel cut oatmeal because of higher protein and fiber content.
- Daily multi-vitamins are OK but avoid the expensive high dose vitamins available in health food stores. They often contain more of a vitamin than the body can absorb.
- Research has not shown up to this point that artificial sweeteners cause cancer. Moderation is key.
- There is no evidence that caffeine causes cancer. It can be an irritant in the GI tract. Up to 4 cups per day is considered OK. Old school recommendation was to not consider coffee and tea as hydration. They are made with water and considered hydration sources.
[email protected]
Disclaimer: The Villages Prostate Group does not recommend or endorse the speakers, publications or descriptions of publications. They are simply provided as additional resources for your information.
