Speaker Summaries (2021)
Monthly Meeting, Dec 1st, 2021
Speaker: Dr. Richard Roach MD, Urologist, Advanced Urology Institute (AUI)
Topic: Erectile Dysfunction (ED)
Our speaker for our in person meeting on Wednesday, Dec. 1, was Dr. Richard Roach, board certified urologist affiliated with Advanced Urology Institute, the biggest urology practice in Florida. His talk focused upon erectile dysfunction (ED).
During sexual arousal impulses from the brain and local nerves cause the muscles of the corpora cavernosa to relax and allowing blood to flow in and fill the open spaces creating pressure on the cavernosa making the penis expand and creating an erection.
ED Definition
Treatments:
Oral drugs which relax certain muscles and blood vessels increasing blood flow to the penis.
Acoustic Wave Therapy involves bombarding the penis with low frequency sound waves. The regimen involves 6 sessions lasting approximately 20 minutes. The treatment is 60 to 70% effective. It is not fully approved by the FDA and Medicare. Costs range from $2,450 to $5,000 depending upon the provider.
Penile Prosthesis
Questions and General Discussion
Fred Barone
[email protected]
Speaker: Dr. Richard Roach MD, Urologist, Advanced Urology Institute (AUI)
Topic: Erectile Dysfunction (ED)
Our speaker for our in person meeting on Wednesday, Dec. 1, was Dr. Richard Roach, board certified urologist affiliated with Advanced Urology Institute, the biggest urology practice in Florida. His talk focused upon erectile dysfunction (ED).
During sexual arousal impulses from the brain and local nerves cause the muscles of the corpora cavernosa to relax and allowing blood to flow in and fill the open spaces creating pressure on the cavernosa making the penis expand and creating an erection.
ED Definition
- ED can be permanent or total where a man cannot form an erection. It can be inconsistent, sometimes one can form an erection and sometimes he cannot. ED can also be considered brief, where one can form an erection but it lasts only briefly. Men can have an orgasm without an erection.
- Spinal Cord Injuries
- Aging: The body's testosterone decreases 10% every decade.
- Lifestyle: Alcohol and smoking
- Chronic diseases: Diabetes and cardiac issues including hardening of the arteries and hypertension.
- Certain medications: Beta Blockers
- Depression
Treatments:
Oral drugs which relax certain muscles and blood vessels increasing blood flow to the penis.
- Viagra taken approximately 30 minutes before needed.
- Cialis taken daily in 5 mg doses. This drug can also increase urine flow and eliminate the need for a drug like Tamsulosin.
- Levitra taken approximately 60 minutes before needed.
- Stendra taken 30 minutes before needed. This drug has shown better results than the above, however, it is not yet generic and costs $60 to $70 per pill.
- Drawbacks include, bleeding, extended erection time, bruising, Peyronie's disease, poor long term results (tendency to lost efficacy overtime), and fear of sticking oneself.
Acoustic Wave Therapy involves bombarding the penis with low frequency sound waves. The regimen involves 6 sessions lasting approximately 20 minutes. The treatment is 60 to 70% effective. It is not fully approved by the FDA and Medicare. Costs range from $2,450 to $5,000 depending upon the provider.
Penile Prosthesis
- This is a surgical procedure that places inflatable or flexible rods into the penis. In addition to the rods, a reservoir holding saline solution and a pump hidden in the scrotum are inserted. Pressing the pump forces saline into the rods giving the man an erection. Repressing the pump brings the saline back up into the reservoir.
- The procedure is performed outpatient under general anesthesia and requires a catheter overnight. Full recovery can take up to two weeks.
- The surgery is covered by Medicare.
- Dr. Roach presented a video showing how the mechanism works. He performs approximately 100 implants per year, down significantly from a prior affiliation where at times he sometimes performed 5 per day. He prefers the Coloplast brand which experience has shown only a 5% leakage after 5 years
- Risks include a) general surgery risks primarily infection and adverse anesthesia reaction; b) erosion of adjacent tissue; c) migration which is movement of the device; d) chronic pain; and e) device malfunction.
Questions and General Discussion
- One man complained of lack of libido after taking casodex in conjunction with radiation therapy. He had libido before the treatment. Advice was to wait several months and then seek treatment if no libido returns.
- One gentleman who had been on intermittent hormone therapy for an extended period of time mentioned that he recently switched to Orgovyx and has had favorable results. Dr. Roach has prescribed this with favorable results.
- Questioned about supplements that would help in inhibiting prostate issues, Roach mentioned Prostate SR, a Saw Palmetto and Beta-Sitosterol supplement. This was developed by 6 of the leading medical centers and universities in the country and inhibits the growth of the prostate and possibly shrinks its size.
- Nocturia is a condition whereby one wakes up during the night to urinate. The antidiuretic hormone in the body wears off with age. A prescription drug, Nocdurna, is a treatment option. However, caution must be taken to avoid sodium washout. Urine will be stored during the night and flushed out in large amounts in the morning which may cause an over excessive voiding of sodium.
- Acidic (coffee, soda, alcohol) and high potassium (tomatoes, avocados, bananas) cause inflammation of the bladder. A mucus lining that protects the walls of the bladder deteriorates with age. Excessive inflammation can overactive bladder issues.
- After radical prostatectomy there is a 5% chance of never regaining bladder control. Roach recommended kegels prior to surgery, 150 per day. For urinary incontinence treatment, Dr. Roach considers reduction to one pad (not diaper) per day successful.
Fred Barone
[email protected]
Monthly Meeting, Oct 6th, 2021
Speaker: Dr. Michael Diaz, MD, Medical Oncologist with Florida Cancer Specialists
Topic: Advocacy and Patients' Rights
Dr. Michael Diaz of Florida Cancer Specialists spoke to our group on Wednesday, Oct. 6,. via Zoom. Dr. Diaz is currently the Assistant Managing Physician for the statewide practice. He serves on the FCS Executive Board and as Director of Patient Advocacy for the practice. In addition to his medical practice, Dr. Diaz provides leadership for a number of organizations, including serving as Chair of the Florida Cancer Specialists Foundation Board of Directors, which offers non-medical financial assistance to qualified cancer patients in Florida. He serves as the Director of Patient Advocacy and Federal Legislative Committee Chair for the Florida Society of Clinical Oncology (FLASCO), as well as being a Past President.
Dr. Diaz' talk focused upon Pharmacy Benefit Managers (PBMs) and some of their practices. PBMs are companies that manage prescription drug benefits on behalf of health insurers, Medicare Part D plans, large companies and other payers.
Questions and Answers
The following two links present animated videos of how PBMs work.
https://www.youtube.com/watch?v=MNKGJG7onSw
https://www.youtube.com/watch?v=YZBWSAFcCrU
For those interested in FLASCO advocacy newsletters or those wishing to be notified of Grass Roots efforts, you can get on the email list here:
https://patients.flasco.org/about-us/contact-us/
The following link goes to another advocacy website that attempts to make an impact in cancer and healthcare policy.
https://communityoncology.org/advocacy/
Speaker: Dr. Michael Diaz, MD, Medical Oncologist with Florida Cancer Specialists
Topic: Advocacy and Patients' Rights
Dr. Michael Diaz of Florida Cancer Specialists spoke to our group on Wednesday, Oct. 6,. via Zoom. Dr. Diaz is currently the Assistant Managing Physician for the statewide practice. He serves on the FCS Executive Board and as Director of Patient Advocacy for the practice. In addition to his medical practice, Dr. Diaz provides leadership for a number of organizations, including serving as Chair of the Florida Cancer Specialists Foundation Board of Directors, which offers non-medical financial assistance to qualified cancer patients in Florida. He serves as the Director of Patient Advocacy and Federal Legislative Committee Chair for the Florida Society of Clinical Oncology (FLASCO), as well as being a Past President.
Dr. Diaz' talk focused upon Pharmacy Benefit Managers (PBMs) and some of their practices. PBMs are companies that manage prescription drug benefits on behalf of health insurers, Medicare Part D plans, large companies and other payers.
- PBMs initially emerged doing nothing more than process claims. As these entities grew, they added more complications to the reimbursement and approval process. The iPBM marketplace has evolved so that now there are three PBMs (CVS, Express Scripts, United Health's Optum) that manage just under 80% of all prescription benefits for everybody in the country. This is just under the government's criteria for a monopoly.
- PBMs have gone to pharmaceutical companies and have negotiated rebates for putting drugs higher up on the recommended que to encourage more use of a particular drug. For new drugs, no matter how good or bad, PBMs will only allow it on the formulary if they get a 50% rebate after the transaction is complete on the back end. PBMs also get a 10% discount on the front end to show the public that the PBMs are saving the public money. This practice inflates the cost of drugs because the pharmaceutical company must incorporate the rebate into the price of drugs.
- Dr. Diaz cited a study that indicated that in 2019 $60 billion went back into middlemen's pockets. These middlemen had nothing to do with patient care.
- Middlemen are not allowed in other countries.
- Indirect Remuneration Fee: Dr. Diaz' practice has an affiliation with a specialty pharmacy which facilitates the delivery of drugs because that pharmacy has access to all the patient's medical records. and can determine if there are any potential problems with a particular prescription. The specialty pharmacy gets paid by the PBM for dispensing the drugs, an amount over the cost of the drug that the pharmacy purchases from the pharmaceutical company or wholesales, allowing the pharmacy to realize a profit. Dr. Diaz' affiliated specialty pharmacy began to notice quarterly adjustments reducing the BM reimbursement by as much as 6% in some cases. The adjustments were for quality measures, even though there are no quality measures for oncology drugs. The affiliated speciality pharmacy was compared to the Southwest Florida region on adherence to blood pressure, diabetes and cholesterol drugs. These fees have now increased to 10 to 12%, and because of the high cost of oncology drugs, they have surpassed an amount in excess of eight digits annually. The specialty pharmacy can be successful in obtaining additional discounts from the manufacturer, but that discount will eventually be included in the price of the drugs.
- PBMs find ways to nickel and dime every component of the system which results in hyperinflation of the cost of drugs. Dir. Diaz estimates that if these rebates and discounts did not exist, the cost of drugs may be 30% to 40% less.
- Step Therapy: PBMs will require that a certain drug be prescribed before the drug that a doctor recommends, either because the drug is more expensive or the rebate is higher.
- For some examples of PBM horror stories on how PBM practices can potentially impact care, access the following link: https://pbmabuses.org/
- Dr. cited an example that one of his partners encountered with a PBM. The patient had metastatic kidney cancer and first line management by the oncologist determined that a certain FDA approved medication was the best treatment. The patient's urologist determined that the patient was not a candidate for surgery. The PBM required surgery before allowing the pill. The PBM made a medical decision, effectively practicing medicine.
- Dr. Diaz is involved with legislative efforts both in Washington and in Florida attempting to bring regulation to the PBMx. Currently, no one in Florida has the legal authority to monitor a PBM. A bill passed the Florida House in the last session giving regulatory authority over PBMs to the Dept. of Insurance. The bill did not reach the Florida Senate until one day before the legislative session ended and therefore no action was taken. PBMs have powerful legislative influence. Dr. Diaz hopes that as the general public becomes more aware of PBM practices, grass root campaigns will eventually lead to lower drug costs and less PBM influence over patient care.
Questions and Answers
- Is there a relationship between PBMs and Medicare Advantage Plans? The answer is complicated since each of the three largest PBMs are under a corporate shell that includes health insurance companies. The inner workings of the two are very difficult to track. Insurance companies can enhance profits by denying benefits. Regular Medicare is not under any corporate shell, but Advantage plans are.
- Is it better to pick one pharmacy over another if the patient has a choice? This often depends upon the person's insurance plan. Often the plan under Medicare will have a high deductible. Dr. Diaz referred to an RX Card and cited an example where one of his patients faced a $500 monthly deductible under her plan, but used an RX Card and achieved a $20 deductible.
- A comment was made regarding purchasing drugs from foreign countries. Dr. Diaz does not recommend this avenue because one cannot be assured of the pedigree of the drug.
- One has the option of asking for a paper prescription and then going to several pharmacies and shopping for the cost.
- How do generic drugs compare to brand name drugs? Dr. Diaz is in favor of generic drugs. Switching to a generic from a brand name drug will be effective 99% of the time. Caution revolves around binders included in the pill. Binders facilitate dissolution of the medication into the stomach or the intestines. Generics will often use different binders and those binders may have adverse side effects.
The following two links present animated videos of how PBMs work.
https://www.youtube.com/watch?v=MNKGJG7onSw
https://www.youtube.com/watch?v=YZBWSAFcCrU
For those interested in FLASCO advocacy newsletters or those wishing to be notified of Grass Roots efforts, you can get on the email list here:
https://patients.flasco.org/about-us/contact-us/
The following link goes to another advocacy website that attempts to make an impact in cancer and healthcare policy.
https://communityoncology.org/advocacy/
Monthly Meeting, Aug 4th, 2021
Speaker: Courtney Lewis, MS, CGD, Genomic Science Liaison for Ambry Genetics.
Topic: Heredity Prostate Cancer and Genetic Counceling
Our speaker on Wednesday August 4 was Courtney Lewis, MS, CGD, Genomic Science Liaison for Ambry Genetics. Her topic was Heredity Prostate Cancer and Genetic Counseling This was our first in person meeting since early March of 2020, and fifteen people attended.
The body is composed of millions of cells, all with a specific purpose. If cells do not function correctly, cancer can develop. All cancer is genetic and some people are born with a higher risk of developing cancer than others.
Prostate cancer can be generally classified into three categories:
The acronym MARY can be used to determine who should test for signs of hereditary cancer.
Genetic Testing can yield one of three results
The key genetic mutation that indicates heredity PCa are the BRCA1 and 2 mutations,
Ambry Genetics and Lake Medical Imaging has entered into a genetic testing program for the detection of gene mutations that could indicate a predisposition to cancer in women. This is known as the CARE program and approximately 22,000 women have taken the initial assessment. 35% of those women have met the NCCN guidelines for genetic testing. Not all in the guideline cohort decided to have additional testing, but of those who did, 7% (approximately 100) were identified to have a positive mutation in a gene that predisposes them to various cancer types. Additional information regarding this program can be obtained by calling 352-326-3823.
Speaker: Courtney Lewis, MS, CGD, Genomic Science Liaison for Ambry Genetics.
Topic: Heredity Prostate Cancer and Genetic Counceling
Our speaker on Wednesday August 4 was Courtney Lewis, MS, CGD, Genomic Science Liaison for Ambry Genetics. Her topic was Heredity Prostate Cancer and Genetic Counseling This was our first in person meeting since early March of 2020, and fifteen people attended.
The body is composed of millions of cells, all with a specific purpose. If cells do not function correctly, cancer can develop. All cancer is genetic and some people are born with a higher risk of developing cancer than others.
Prostate cancer can be generally classified into three categories:
- Sporadic which encompasses 70 to 80% of the cases. These are cancers that occur by chance in one or two family members that are not due to an inherited gene mutation.
- Familial which encompasses 15 to 20% of the cases. These result from a pattern or related types of cancer within a family that may be due to genes and/or other shared factors, such as environment and lifestyle.
- Hereditary which encompasses 5 to 10% of the cases. These are cancers with the same patterns or related types within a family due to inherited gene mutations that can be passed from parent to child.
The acronym MARY can be used to determine who should test for signs of hereditary cancer.
- Multiple: Two or more primary cancers in the same person; three or more same or related cancers on the same side of the family; 10 or more colorectal polyps in a patients lifetime.
- Ancestry: Family history of breast or pancreatic cancer.
- Rare: male breast cancer; ovarian cancer; pancreatic cancer; metastatic prostate cancer.
- Young: any of the following cancers diagnosed <50 years of age: breast, colorectal, uterine.
Genetic Testing can yield one of three results
- Positive: A mutation was detected in at least one of the genes tested which is associated with an increased risk of developing certain types of cancer. This has medical management implications.
- Negative: no mutations were detected in the genes that were tested. The patient should be managed based on personal and family history.
- Variant of Unknown Significance (VUS): A genetic variant was identified in at least one of the genes tested, however, there is insufficient evidence for this to be linked to an increased risk of developing cancer. The results may change over time as more information becomes available through further testing.
The key genetic mutation that indicates heredity PCa are the BRCA1 and 2 mutations,
- Ambry Genetics normal cohort consists of tests for mutations for 36 genes, 10 of which are linked to increased lifetime risk for prostate cancer.
- BRCA 1 and BRCA 2 were originally associated with breast cancer but also impact PCa, These mutations are important because 1) data suggests these mutations are associated with more aggressive PCa and 2) there is a 50/50 random chance that the patient's offspring will have the same mutation.
- In one active active surveillance study, 42% of men with either BRCA or ATM mutations had grade reclassification vs 23% of non-carriers of these mutations.
- One of the facilitators in the meeting referenced a recent webinar produced by US Too International featuring Dr. Laurence Klotz of Toronto, CA. Dr. Klotz is well known in the realm of PCa treatment and a big proponent of active surveillance given the proper low risk diagnosis. In his video he recommends against active surveillance for patients with BRCA mutations because of their explosive nature for the acquisition of genetic aberrations. The timeline for PCa progression is normally much longer for PCa caused by other mutations.
- NCCN Guidelines report that early studies indicate there may be a clinical benefit of poly-ADP ribose polymerase (PARP) inhibitors for PCa patients with BRCA mutations.
Ambry Genetics and Lake Medical Imaging has entered into a genetic testing program for the detection of gene mutations that could indicate a predisposition to cancer in women. This is known as the CARE program and approximately 22,000 women have taken the initial assessment. 35% of those women have met the NCCN guidelines for genetic testing. Not all in the guideline cohort decided to have additional testing, but of those who did, 7% (approximately 100) were identified to have a positive mutation in a gene that predisposes them to various cancer types. Additional information regarding this program can be obtained by calling 352-326-3823.
Monthly Meeting, June 2nd, 2021
Speaker: Dr. Chiedozie A. Mkpolulu, MD, Radiologist, Lake Medical Imaging
Questions and Answers
Speaker: Dr. Chiedozie A. Mkpolulu, MD, Radiologist, Lake Medical Imaging
- Dr. Tony initiated the discussion by providing background information about LMI. The practice has 22 Board Certified Radiologists on staff and will have 26 by the end of July. The practice is fully accredited by the American College of Radiology. and has been serving the community for over 50 years. LMI has a diagnostic center in Leesburg and five in The Villages. LMI opened a center in the Advanced Healthcare Facility in the Brownwood area. This is a 20k square foot full service center with a 3T MRI, 160 slice CT and 2 3D mammo units. The center also performs LVI procedures, fluoroscopy, X-ray and US/Echo procedures.
- Prostate Cancer (PCa) is the most common malignant cancer in men, the second most common cause of cancer death after lung cancer, has a lifetime risk of 1 in six men in developed countries, and has a median age of 68 at diagnosis.
- Regarding diagnosis, Dr. T showed a graphic of a DRE, posited that a normal PSA is < 4ng. ml, that with age, PSA rises and 6.5 ng ml. is acceptable for men > 70 but a rise of .75 ng.ml. in a 12 month period is cause for concern.
- Transrectal Ultrasound Biopsies (TRUS) are often flawed in that samples are obtained by random needle snips. This can often lead to missing cancer cells. Hence the need to pinpoint a suspicious lesion in the gland and directly biopsy it.
- Studies showed that prostate MRI improves the process of triaging patients for biopsy and helps to detect suspicious lesions, determine localization, characterize the nature, stratify risk, provide surveillance, assess potential recurrence and provide image guided biopsies.
- MRI's are widely accepted as a process in diagnosing PCa. Images are graded using the Prostate Imaging and Reporting and Data System (PI RADS). PI RADS are presented in a 1 to 5 scale, with 1 being highly unlikely that significant cancer is present and 5 being highly likely that significant cancer is present. PI RADS 4 and 5 indicate the need for a biopsy.
- There are two types of MRI's, multiparametric (MpMRI)and biparametric. (BpMRI)
- MpMRI refers to the use of multiple magnetic resonance imaging parameters to supplement the imaging. The components are T2 weighted imaging (T2WT), dynamic contrast enhanced (DCF) MRI and diffusion-weighted imaging (DWI).
- BpMRI uses just two parameters in providing an image, T2WT and DWI. Radiologists do not inject contrast into the patient when performing a BpMRI image.
- GFR is a measure of kidney filtering capacity. If a person has a GFR of 50, that means his kidneys are filtering at 50% of normal. Patients with a GFR of < 30 cannot have MpMRI images because of the contrast agent.
- MpMRI provides sharper images than BpMRI. In intermediate cases, intravenous contrast enhancement often increases the PI RAD 3, intermediate suspicious to PI RAD 4; highly suspicious.
- There is no magic number for the smallest lesion that can be detected by MpMRI. Lesions as small as 5 millimeters can be detected
- Patients must wait six weeks after a biopsy to have an MpMRI because of inflammation to the gland. Sometimes an enema is required to reduce artifacts of stool in the rectum. To reduce artifacts from bowel peristalsis, an antispasmodic agent such as glucagon or scopolamine may be required. Patients should refrain from ejaculation three days prior to the MRI to maintain maximum distension of the seminal vesicles. .
- Pacemakers: Patients with pacemakers can get an MRI but only using a 1.5T magnet, not a 3T magnet. The pacemaker must be FDA approved and MRI compatible. The imaging must take place at a location near a hospital. Off-brand pacemakers preclude the patient from receiving an MRI and if the practicing radiologist cannot confirm that the pacemaker is MRI compatible, he cannot perform an MRI
- Gadolinium is the intravenous contrast used and it is safe for adults. Patients must have a healthy function, preferably a GFR > 60 since kidneys do the work of flushing out gadolinium within 24 hours after injection. For patients with a GFR <60 but > 35, radiologists can still use gadolinium, but normally inject a half dose. With a GFR < 30, no contrast is used because of the risk of Nephrogenic Systemic Fibrosis (NSF).Common mild side effects of gadolinium include pain at the injection site, nausea, itching, rash, headaches and dizziness. Rare moderate to severe side effects include difficulty breathing and swelling of the lips and mouth. Board certified physicians are always on site to monitor and treat. There is evidence that some types of gadolinium based agents may predispose to NSF than others. LMI uses Prohance - Gadoteridol which shows a very low association with NSF. A very small amount of gadolinium may be retained in body tissue, mostly in the bones with a tiny amount in the brain. At this stage, there are no known adverse effects from the very small amounts of retained gadolinium.
- MpMRI/Ultrasound Fusion Biopsy: For decades, prostate biopsies were performed using ultrasound guidance and utilized random sampling collecting 12 to 24 samples. Now, radiologists use a newer 3D technology to map out the suspicious lesion on MP. Maps are then fused with Ultrasound and the area of concern is easily identified and the needle is directed to the specific spot. This improves the accuracy of the biopsy.
- Cases: Dr. Tony presented a series of slides showing images of the prostate and the surrounding pelvic area. Using a pointer he highlighted the cancerous lesions on the images. These included examples of lesions contained in the gland and cancerous cells spread into the seminal vesicles, bladder and lymph nodes. Very informative.
Questions and Answers
- Why isn't an MpMRI standard practice before having a biopsy performed? The trend now is to have an MpMRI and then a fusion biopsy. This is becoming normal practice and insurance companies are increasingly covering the MpMRI. One audience member stated that he recently had to absorb a co-pay of $185 for a BpMRI. The writers of this summary shared his experience. In 2016, his urologist ordered an MpMRI and his insurance would not pay for it. Iin 2018, the urologist ordered another MpMRI, and insurance covered all but a $66 co-pay.Evidence that the trend is that insurance companies are covering the imaging.
- What is the full range of PSA readings? Dr. Tony stated that he did not know of a "full" range. Some are very very low and some are very very high. Dr. has no fixed number. One member stated that he heard of PSA readings in the thousands.
- Does an MRI include an image of the anterior portion of the prostate? An MRI provides an image of the entire prostate gland and therefore includes the anterior area. If a lesion appears in this area, a transperineal biopsy is required to determine the severity of the lesion.
- If after age 70, the 6.5 ng ml is the acceptable level, as a person ages, does the acceptable level increase? The answer is no. Rate of increase is the focus after age 70.
- If a patient has a very low PSA starting point, does a rate of increase less than 0.75 become a concern? Studies show that the .75 figure remains constant. However, after a patient has had an intervention, his urologist may request an annual MRI.
- Can a primary care physician order an MRI? Yes.
- A question was asked regarding the meaning of a PI RAD reading of 3/4. Dr. stated that was probably a reading from a BpMRI With contrast, a radiologist should be able to specifically grade the tumor as either 3 or 4.
- If a small tumor appears on a biopsy, and then no tumor appears on a subsequent MRI, would there be a reason to do another biopsy? If no cancer is found, there can be no mapping and therefore the inability to do a fusion biopsy.
- There are drugs that slow down the movement of the bowel. Is it standard practice to prescribe these drugs with MRI's? It is not standard. At LMI, when the imaging starts, the radiologist will be able to visualize the movement of the bowel and determine if the drug is necessary? The drug is administered intravenously
- The same mapping process is used for transperineal and transrectal biopsies.
Monthly Meeting, May 5th, 2021
No Speaker.
We played a video presented by the Active Surveillance Patients International (ASPI) support group on April 24th of this year. The presentation focused upon Transperineal Biopsies (TP) and favored them over Transrectal Biopsies (TR). Sepsis and resulting complication are a prime concerns with TR biopsies, and the risk of sepsis is significantly reduced with TP. You can view the video at the link below.
https://www.youtube.com/watch?v=hod3-SUoAw8
The speakers on the video are:
https://www.youtube.com/watch?v=NIi-xLPfGNM&t=9s
We had an interesting discussion towards the end of our meeting. One attendee stated that he battled AUR after his TP and went to the emergency room for treatment. Insertion of a catheter provided immediate relief. After the second incident, doctors taught him how to self insert, which he did for less than a week when the problem ceased. He stated that he had a "saturation" TP with 57 specimens taken. He deducted that this was an excessive amount of trauma to the prostate and should he need another biopsy, he would again opt for TP, but limit the number of cores. Another participant stated that he had a TP and at the time of the procedure, the doctor taught him how to self insert and that it is not difficult to do. He used a catheter for only a couple of days.
No Speaker.
We played a video presented by the Active Surveillance Patients International (ASPI) support group on April 24th of this year. The presentation focused upon Transperineal Biopsies (TP) and favored them over Transrectal Biopsies (TR). Sepsis and resulting complication are a prime concerns with TR biopsies, and the risk of sepsis is significantly reduced with TP. You can view the video at the link below.
https://www.youtube.com/watch?v=hod3-SUoAw8
The speakers on the video are:
- Dr. Ricard Szabo, an urologist affiliated with the University of California, Irvine. His talk starts at the 4:00 minute mark of the video. Dr. Szabo 1) presented graphics showing the different needle positions between TP and TR, 2) presented the dangers of Sepsis, 3) posited that TR biopsies are inaccurate and dangerous because of antimicrobial resistance, 4) presented statistics showing death from TR, 5) estimated that 39,000 cases of sepsis per year would result from the approximately 2 million TR biopsies performed in the US this year, and projected the hospitalization cost between $341 million and $752 million 6) referred to a study that TP coupled with MRI/ultrasound fusion targeting yielded clinically significant cancer 50% to 60% greater than MRI/ultrasound fusion target than with TR, 7) referenced a study that showed that TP is significantly better is discovering hidden cancers in men on active surveillance, 8) mentioned that rectal bleeding will not happen with TP, 9) talked about misconceptions regarding TP: perceived need for general anesthesia, increase costs, procedure time much longer, increased pain and then presented evidence refuting each of those misconceptions, 10) concluded that TP is more accurate, safer, and less costly than TR.
- Dr. Rick Popert, Consultant Urological Surgeon, Guy's and St. Thomas NHS Foundation Trust, London. Dr. Popert 1) reviewed the evolution of the standard of care over the last twenty years, 2) referred to the rectum as a dirty box and prostate as a clean box, 3) talked the incidences of fever and sepsis related to TR and stated that the because of the resistance of bacteria to antibiotics, one cannot prescribe a fool proof antibiotic, 4) discussed a patient that developed sepsis in 2005 from a TR that significantly altered that patient's lifestyle and lead to Popert doing TP in 2006, 5) presented the stratification for patients qualifying for TP in 2006, 6) presented statistics of 709 TP cases from 2007 -2012 showing that 63 of 174 who had prior negative biopsies had cancer, that 131 of 350 thought suitable for AS had a higher grade or volume of disease and that 116 out of 185 having their initial TP biopsy had cancer, 15% of which were in the anterior sector exclusively, 7) stated that the European Association of Urology stated in their guidance that prostate biopsies should be TP because of the possibility of sepsis, 8) of the 709 cases mentioned in #6, there were no cases of urosepsis, 11 cases of Acute Urinary Retention (AUR), two of which were assiciated with blood clots, 2 were hospitalied with hematuria and settled with conservative measures, and a total of 9 cases were hospitalized with management of complications, 9) referred to the Precision Point Transperineal Access System (PPBX) and stated this allowed him to perform TP effectively under local anesthesia, 10) showed a very interesting video whereby he performed a TP under local anesthesia using the PPBx, 11) presented that in September 2017, the urologists at Guy's hospital closed the door on TR using the term TREXIT and embarked upon an endeavor to have all hospitals in the UK to convert to TP.
- Junah Busere, urological nurse at Guy's hospital. This speaker talked about the training that he received to become qualified to perform TP using the PPBx. I did not show this portion of the video because it did not present anything that would promote our understanding of TP.
- Dr. Mathew Allaway, Urologist and inventor of PPBx. Dr. Allaway's presentation starts a the 58th minute of the video, he 1) stated that back in the 1970's and early 1980's, urologists were performing biopsies through the perineum, but procedures were very crude and the doctor guided the needle by feel of the prostate, 2) that ultrasound technology gave urologists the ability to see what they were biopsying, but the technology was not sufficient enough to allow doctors to go through the perineum, 3) revealed that infection and missed cancer were the motivators to develop his product and discussed the problems with TP before he developed his product, 4) stated that his PPBx is a free hand approached, 5) faced criticism in 2014 for the PPBx at that time, 6) took three more years to develop PPBx which was the first class 2 product approved for TP, 7) showed a graphic of a test result of 179 men that reflected 79% overall cancer detection, 61% detection with PiRad 1&2, no sepsis, 8) presented a color coded graphic of the prostate that showed regions that cannot be reached with TR, 9) emphasized the importance of training and presented a speeded-up video of his training video.
https://www.youtube.com/watch?v=NIi-xLPfGNM&t=9s
We had an interesting discussion towards the end of our meeting. One attendee stated that he battled AUR after his TP and went to the emergency room for treatment. Insertion of a catheter provided immediate relief. After the second incident, doctors taught him how to self insert, which he did for less than a week when the problem ceased. He stated that he had a "saturation" TP with 57 specimens taken. He deducted that this was an excessive amount of trauma to the prostate and should he need another biopsy, he would again opt for TP, but limit the number of cores. Another participant stated that he had a TP and at the time of the procedure, the doctor taught him how to self insert and that it is not difficult to do. He used a catheter for only a couple of days.
Monthly Meeting, April 7, 2021
Dr. Cathleen Civiello, PhD., Clinical and Organizational Psychologist, Simed Health
Dr. Cathleen Civiello, PhD. delivered our presentation via Zoom on Wednesday, April 7. Dr. Civiello is a clinical and organizational psychologist with over 33 years experience. She is certified by the and is affiliated with Simed Health, a multi-specialty organization with over 150 medical professionals. Her talk was titled Surviving: Covid-19 and Cancer.
Stress Overview
Yoga: https://carynmartinwellness.com/
Support Resources
Cancer Resources
[email protected]
Dr. Cathleen Civiello, PhD., Clinical and Organizational Psychologist, Simed Health
Dr. Cathleen Civiello, PhD. delivered our presentation via Zoom on Wednesday, April 7. Dr. Civiello is a clinical and organizational psychologist with over 33 years experience. She is certified by the and is affiliated with Simed Health, a multi-specialty organization with over 150 medical professionals. Her talk was titled Surviving: Covid-19 and Cancer.
Stress Overview
- Autonomic Nervous System (ANS) Why does the brain stop working in the doctor's office?
- The Sympathetic Nervous System (SNS) Mode is designed to turn on to a significant life stresser, i.e. a bear or lion. Fight or Flight. ANS has not evolved the way stressors in our environment have evolved. SNS stays on longer than intended. When it turns on, things not needed in Fight or Flight turn off, like your brain or gut processing. You don't remember what happened.
- Tools to combat this: 1) Take a second set of ears to the Doctor's office; Many doctors now only allow the patient in the room; request using the phone function so that the second set of ears can participate. If using telehealth, request that a second set of ears be present. 2) Prepare for the appointment in advance. Make three copies of your questions, one for you, one for the doc and one for the second set of ears. 3) Develop a relationship with the doctor's staff. Many are difficult to deal with, but treating them nicely will often result in you getting what you want. 4) Breathe deeply. Body in stress often demonstrates shallow breathing. Deep breaths tell the brain that the stress is over and it can start function again. 4) 5 Senses Tool. This is your mind going through your five senses. What am I hearing now? Chatter outside the room; X-ray machine: What do you feel, cold or warm? Smell anything? This can anchor you and turn off the Fight or Flight mechanism.
- Other Tools Not in the MD's Office (What happens when I go back out? Will people be breathing Covid on me?)
- Imagery: Find a place that is relaxing to you and in your five senses, go back to that place and imagine it.
- Progressive Muscle Relaxation: go to different parts of the body and tensing and relaxing those parts.
- Breathing: Inhale for a 4 count; Hold for a 7 count; Exhale for an 8 count. Helpful because it takes brain power as well as physiological power.
- Exercise is critical. It benefits physical health and mental health. One of the most effective tools in overcoming anxiety and depression. Exercising outside has an additional benefit. Just being outside has a positive effect on cancer outcomes.
- Distraction: Structured day. Because of Covid, many people had to forego regularly scheduled activities. Part of the anxiety of Covid is the lack of structure.
- Intentional writing. This tool involves writing down what is bothering the writer and then tearing up the paper. Write, don't type. Good tool to fall asleep.
- Meditation. focus the brain to concentrate on something external.
- An audience member posed the question: When I am stressed, I read and the stress goes away. Why is that? Reading is a combination of distraction and imagery. Also when people read they tend to be psychologically immersed. This is a three pronged benefit to overcome anxiety.
- Someone or Something to love. Could be a pet or someone you check in with every day
- Something to do. Be Busy. Develop a structure
- Something to look forward to. Does not have to be major. Hardest thing in the Covid crisis. People lost things that they looked forward to.
- People with cancer should talk about living with cancer, not dying from it.
- No is a complete sentence. No one knows your health status as well as you do. Don't let anyone guilt you into something you do not want to do or are unable to do.
- In person or telehealth. Depends on each circumstance
- Beware of the internet. Utilize reputable sites.
- Talk about the tough stuff with both your physician and your partners, i.e. sex
- Follow up important after treatment.
- The Villages are opening up, but doctors are still recommending CDC guidelines or even more strict COVID guidelines. Groups starting up again. Pressure from neighbors and friends to participate in social gatherings. What to do?
- Verbally assaulted at mailbox for wearing a mask.
- People are being bored, alone and isolated causing anxiety.
- People gaining or losing weight because of unhealthy eating and drinking habits
- Books and audio. Local libraries are accommodating
- Museums you can tour virtually. Virtual Museum
- Great Courses https://www.thegreatcourses.com/ Costs vary by course or $20 per month for all courses in the catalogue
- Master Classes: $180 per year; https://www.masterclass.com/
- Travel https://thingstododc.com/ and https://www.roadscholar.org/
- Profession or former profession
- Coursera.org offers free courses.
Yoga: https://carynmartinwellness.com/
Support Resources
- Support groups like our support group
- Faith Community: If your community is doing things that are uncomfortable, try a different one
- TLC Services, a partner of the United Way https://tlc-services.org/
- Grief: https://www.griefshare.org/about/online
- AA: https://www.onlinegroupaa.org/
Cancer Resources
- Overall best resource in Cathleen's opinion: https://www.cancer.org/
- What To Ask Your Physician: Questions Prostate
- The Take From Mayo: MayoClinicProstate
- For Caregivers and Family: https://www.cancer.org/treatment/caregivers.html
- Questions About Sex: Sexual Issues
- Is there a link between nutritional health and psychological health? Answer: Cathleen stated that she is not the right person to address this issue. She has not seen the good, but has seen the bad where poor nutrition is detrimental to psychological health.
- Attitude: There are many things that cause stress that one has no control over. There is one thing that anyone can control daily, even though it is very difficult at times. That is one's attitude. Answer: If you find yourself saying the word "should" because you are not doing important things, that is a clue of poor attitude. Do something positive every day, no matter how small or seemingly insignificant. One member of the audience offered what he called self programming each morning by telling yourself that you are going to have a great day. works for him. He stated that you must say it out loud. A retired professional athlete in the audience offered that pro athletes are taught to face a mirror in the morning and ask yourself if you are going to have a good day or a bad day. This procedure worked for him.
- Cathleen offered a technique for going to bed at night. Self talk your way through a dream that you want to happen.
- One member who is on hormone therapy shared his experience with fatigue. Anxiety because he cannot do the things he is accustomed to doing. He has learned to set limits and stop what he is doing before he reaches his body limit. Answer: Cathleen reiterated the importance of listening to your body.
- A person stated that he is a sculptor by trade and has all the tools to create sculptures, but has not done anything since Covid hit. Answer: Cathleen stated that this is not uncommon. People will get back to doing things. She used the term "Reentry".
- Exercise combats fatigue, but is difficult to do when tired. One suggestion from the audience was to work out in a pool. Your body weighs much less in water and you are able to do more. Answer: Cathleen stated that pool exercises are wonderful but cautioned to not exercise until you are tired. It is easy to overdo it, become overly fatigued and fail to continue exercising.
[email protected]
Monthly Meeting, March 3, 2021
Roxanne Mennello, MS, R.T.(R)(M), Clinical Account Specialist, Profound Medical
Our speaker for our virtual meeting on Wednesday, March 3, was Roxanne Mennello, clinical account specialists for Profound Medical. Roxanne was joined by two clinical scientists, Amanda Bessarra and Nathan Soucier, also from Profound. Profound developed a procedure known as TULSA-PRO, (Transurethral ULtra Sound Ablation of the PROtate). This is a relatively new procedure having received FDA approval in August of 2019.
Roxanne started her talk with a graphic overview of the anatomy of the prostate and surrounding pelvic area and a brief discussion of PSA. She also presented statistics regarding PCa, 1 in 9 men), the importance of risk factors (genetics, age, race, etc.) and the importance for each patient to understand his personal risk because not one size fits all. She also talked briefly about BPH, an enlarged prostate which can cause elevated PSA but is not cancerous.
Current Standards of Care:
TULSA
Procedure:
Roxanne Mennello, MS, R.T.(R)(M), Clinical Account Specialist, Profound Medical
Our speaker for our virtual meeting on Wednesday, March 3, was Roxanne Mennello, clinical account specialists for Profound Medical. Roxanne was joined by two clinical scientists, Amanda Bessarra and Nathan Soucier, also from Profound. Profound developed a procedure known as TULSA-PRO, (Transurethral ULtra Sound Ablation of the PROtate). This is a relatively new procedure having received FDA approval in August of 2019.
Roxanne started her talk with a graphic overview of the anatomy of the prostate and surrounding pelvic area and a brief discussion of PSA. She also presented statistics regarding PCa, 1 in 9 men), the importance of risk factors (genetics, age, race, etc.) and the importance for each patient to understand his personal risk because not one size fits all. She also talked briefly about BPH, an enlarged prostate which can cause elevated PSA but is not cancerous.
Current Standards of Care:
- Active Surveillance: psychological stress and can cost up to $29,000 over a 10 yr period
- Radiation: high rates of side effects, 30% of patients fail treatment
- Radical Prostatectomy: removal of whole gland, 85% of patients experience side effects, relatively longer recovery time
- Others: cryotherapy, HIFU, Brachytherapy, and TULSA: whole gland and focal therapy treatments
TULSA
- Transurethral: through the urethra: No incision needed. No energy through the rectum
- Ultrasound: high frequency sound waves used in medical imaging: Waves are increased to produce cell death; minimal damage to surrounding tissue
- Thermal: relating to heat: Prostate tissue is heated to the point of ablation
- Ablation: destruction or removal of tissue: Whole gland or targeted death of tissue cells.
- MRI: medical imaging using a strong magnet: Technique used to image anatomy and physiology
- Closed Loop Feed Back: continuous temperature with real time reading: Physician can see tissue temperature every six seconds.
- Procedure takes 2 to 4 hours depending upon circumstances, but the ablation time takes about 45 minutes
Procedure:
- Preparation (longest time) involves MRI screening, anesthesia, catheter insertion, quality assurance checks on the equipment
- Planning: physician will create a treatment plan based upon MRI imaging, anatomy and treatment needs. Involves outlining the target area on the image.
- Treatment: automated and robotically driven adaptive therapy delivery
- Confirmation: physician will confirm intended areas of the prostate have been ablated. Prostate will probably swell two to three weeks after treatment
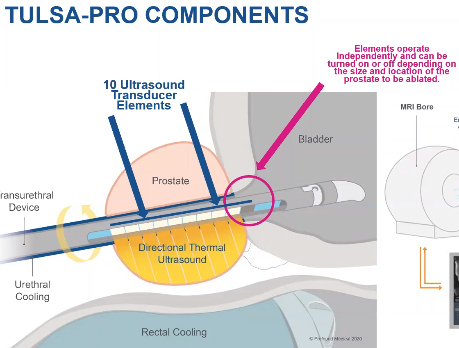
Components:
Erectile Dysfunction 23% 79% 63% 58%
Urinary Incontinence 2.6% 15% 4% 3%
Urethral Stricture 2.6% 9% 2% 35%
Gastro-Intestinal Toxicity 0% 15% 25% 7%
After the Procedure
Q: Is there any limit regarding the size of the prostate that prohibits this procedure?
A: The procedure has been performed on patients with a prostate as high as 250cc's. The location of the lesion and proximity to the rectum are important considerations.
Q: Can the procedure be performed after radiation?
A: The FDA approval is for Prostate Tissue Ablation, not just for treating prostate cancer. In Europe, urologists have used TULSA for salvage after radiation. It can also be used to treat BPH.
Q: Can the procedure be used to treat cancer cells outside the prostate?
A: Typically the procedure is used to treat only cancer cells in the prostate capsule. However, one of the clinical scientists has seen it used to treat cells in the seminal vesicles. The Ultra Sound originates in the center of the prostate and travels outward and has a weakened effect as it travels outside the prostate.
Q: Since TULSA can be used to treat BPH, how does the procedure compare to REZUM?
A: If there is suspicion of cancer, TULSA will treat the cancer along with the BPH in one treatment. Also, TULSA has real time temperature control which REZUM does not.
Q: What are the chances of recurrence?
A: 80% of the men in the clinical trial received a histological benefit after one year. 7% of the men underwent additional treatment after two years.
Q: Is the procedure covered by Medicare at the present time?
A: There is no CPT code at the present. Profound Medical is working on a pathway with a goal of obtaining such a code by 2023. Costs have ranged from $25,000 to $35,000. In some instances, certain treatment centers have been successful by using code C9734 for focused ultrasound therapeutic intervention to obtain partial reimbursement. However, this reimbursement has not been successful across the board.
Q: How much of the prostate will be ablated?
A: This depends upon the size and location of the lesion. This is normally a shared decision between the physician and the patient. Some patients may want whole gland ablation even thought there is only a small, well defined lesion.
Q: In a total gland ablation situation, can the procedure spare the surrounding nerve bundle?
A: Yes. The physician can target the procedure to stop short of the bundle.
Q: How many procedures have been performed to date?
A: In 2020, 1,000 patients worldwide.
- The transurethral device device contains 10 transducer elements which deliver energy into the prostate with the tip of the device ending in the bladder. If the patient is receiving a whole gland treatment, all ten transducer elements are employed, if focal, a lesser amount. Heating can go up to 55 degrees. A fluid management system provides cooling to the transurethral device and also to another probe that is inserted into the rectum. to protect surrounding tissue. The portion of the transurethral device rotates counterclockwise until either the target area or the entire gland is ablated. This movement is robotically controlled.
Erectile Dysfunction 23% 79% 63% 58%
Urinary Incontinence 2.6% 15% 4% 3%
Urethral Stricture 2.6% 9% 2% 35%
Gastro-Intestinal Toxicity 0% 15% 25% 7%
After the Procedure
- Medication, including antibiotics, procedure success and follow up tests (PSA) will be determined by physician assessment
- Catheter: The prostate swells after the TULSA procedure and the physician will utilize a catheter to insure urine flow. The bigger the size of the ablation, the longer the catheter must remain in place. For a full gland treatment, the catheter normally remains in place 10 to 14 days.
- Recovery time: Patients typically return to daily activities, including work, within a couple of days and then to baseline urinary/bowel quality of life within three months
- Eligible for MRI imaging
- Assessed by an anesthesiologist
- Personalized risk assessment (PSA, Gleason, Prostate Size, Location of lesion withing the prostate, etc.) performed by treating physician. In clinical trials, the patient population consisted of men with low and intermediate risk, organ confined PCa.
- Go to tulsaprocedure.com to find worldwide treatment centers. In Florida, two urologists perform this procedure, Dr. Stephen Scionti in Sarasota and Dr. Chandler Dora affiliated with the Mayo Clinic in Jacksonville.
Q: Is there any limit regarding the size of the prostate that prohibits this procedure?
A: The procedure has been performed on patients with a prostate as high as 250cc's. The location of the lesion and proximity to the rectum are important considerations.
Q: Can the procedure be performed after radiation?
A: The FDA approval is for Prostate Tissue Ablation, not just for treating prostate cancer. In Europe, urologists have used TULSA for salvage after radiation. It can also be used to treat BPH.
Q: Can the procedure be used to treat cancer cells outside the prostate?
A: Typically the procedure is used to treat only cancer cells in the prostate capsule. However, one of the clinical scientists has seen it used to treat cells in the seminal vesicles. The Ultra Sound originates in the center of the prostate and travels outward and has a weakened effect as it travels outside the prostate.
Q: Since TULSA can be used to treat BPH, how does the procedure compare to REZUM?
A: If there is suspicion of cancer, TULSA will treat the cancer along with the BPH in one treatment. Also, TULSA has real time temperature control which REZUM does not.
Q: What are the chances of recurrence?
A: 80% of the men in the clinical trial received a histological benefit after one year. 7% of the men underwent additional treatment after two years.
Q: Is the procedure covered by Medicare at the present time?
A: There is no CPT code at the present. Profound Medical is working on a pathway with a goal of obtaining such a code by 2023. Costs have ranged from $25,000 to $35,000. In some instances, certain treatment centers have been successful by using code C9734 for focused ultrasound therapeutic intervention to obtain partial reimbursement. However, this reimbursement has not been successful across the board.
Q: How much of the prostate will be ablated?
A: This depends upon the size and location of the lesion. This is normally a shared decision between the physician and the patient. Some patients may want whole gland ablation even thought there is only a small, well defined lesion.
Q: In a total gland ablation situation, can the procedure spare the surrounding nerve bundle?
A: Yes. The physician can target the procedure to stop short of the bundle.
Q: How many procedures have been performed to date?
A: In 2020, 1,000 patients worldwide.

Monthly Meeting, February 3, 2021
Dr. Adewale Fawole, Board Certified Oncologist, Florida Cancer Specialists,
Our speaker for our meeting on February 3 was Dr. Adewale Fawole. He is a board-certified Hematologist, and Medical Oncologist. He completed his internal medicine residency at the Cleveland Clinic.and then pursued a fellowship in Hematology and Medical Oncology at Oakland University William Beaumont School of Medicine in Michigan. He is currently affiliated with Florida Cancer Specialists and has over 20 years experience.
Genetic Testing. Dr. Fawole recommends germline genetic testing for anyone with prostate cancer (PCa) and the following:
Targeted Therapies, an example of knowing the underlying problems and using that knowledge to treat patients.
Relugolix
Dr. Adewale Fawole, Board Certified Oncologist, Florida Cancer Specialists,
Our speaker for our meeting on February 3 was Dr. Adewale Fawole. He is a board-certified Hematologist, and Medical Oncologist. He completed his internal medicine residency at the Cleveland Clinic.and then pursued a fellowship in Hematology and Medical Oncology at Oakland University William Beaumont School of Medicine in Michigan. He is currently affiliated with Florida Cancer Specialists and has over 20 years experience.
Genetic Testing. Dr. Fawole recommends germline genetic testing for anyone with prostate cancer (PCa) and the following:
- High-risk, very high-risk, regional or metastatic PCa
- Ashkenazi Jewish ancestry
- Family history of high risk germline mutations, eg. BRCA 1/2, Lynch mutation
- A positive family history of cancer: A strong family history of prostate cancer consists of: brother or father or multiple family members who were diagnosed with prostate cancer (but no clinically localized Grad Group 1 (GG 1)) at < 60 years of age or who died from PCa or > or equal to 3 cancers on the same side of the family, especially < 50 years of age; bile duct, breast colorectal, endometrial gastric, kidney, melanoma, ovarian, pancreatic, PCa but not GG 1 or small bowel or urothelial.
- DNA damage occurs everyday and our bodies have a unique way of repairing that damage. When there is a problem with the repair process, that usually leads to cancer. Microscopic views can determine genetic instability. Genetic testing for germline variants should include MLH1, MSH2, MSH6 and PMS2 and homologous recombination genes BRCA 1&2, ATM, PALB2, and CHEK2. The more we know about genetic issues, the more we can develop drugs to attack those issues. Dr. stressed the importance of genetic counseling for patients undergoing treatment based upon genetic testing discoveries.
- Not all patients should have genetic tests performed, only those who meet screening guidelines. Testing everybody would be a waste of time and money and would not provide useful information.
Targeted Therapies, an example of knowing the underlying problems and using that knowledge to treat patients.
- In May of 2020, the FDA approved the poly (ADP-ribose) polymerase (PARP) inhibitors Rucaparib and Olaparib as the first targeted therapies in biomarker-preselected patients with metastatic castration-resistant prostate cancer.
- This provided new options for patients with deleterious BRCA1 or BrCA2 mutations (both drugs), or with deleterious mutations in one of a number of homologous recombination repair genes (olaparib).
- When androgen deprivation therapy is no longer effective because of gene mutations, these drugs provide another line of treatment that may be effective in lieu of chemotherapy. Objective is to treat the cancer cells, not harm good cells.
Relugolix
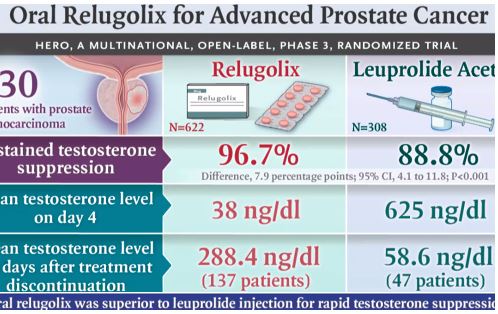
- Relugolix is a recently FDA approved gonadotropin-releasing hormone antagonist.
- In the HERO phase 3 clinical trial, Relugolix was compared to Lupron for 48 weeks. Relugolix is taken orally whereas Lupron requires injections. The primary end point of the trial was sustained testosterone suppression to castrate levels (<50 ng per deciliter) through 48 weeks.
- Summary Results:
- This study is proof of concept that the pill actually works. Dr. Fawole stated that in his field, practitioners like to have multiple studies that a concept actually works.
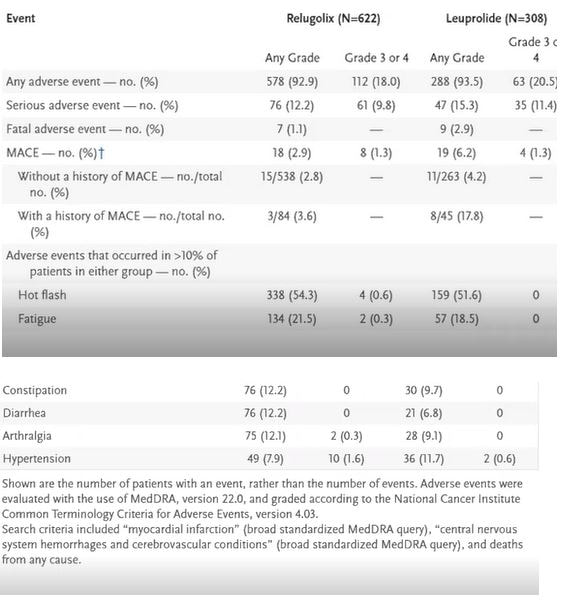
- Side Effects : Among the patients the incidence of adverse cardiovascular events was 2.9% in the Relugolix group compared to 6.2% in the Leuprolide group. Below is a comparison of other side effects:
SpaceOar
- Dr. Fawole talked about SpaceOar. I am not going to present his comments other than to say it is an important part of radiation therapy. Many of our other speakers have spoken about this hydrogel and I have documented those comments in summaries of those speakers.
- Benefit vs. Adverse Effects of Relugolix: As the chart above shows, adverse effects are comparable, some better, some worse. The benefits are faster reduction of testosterone and for those who have mobility issues, the ability to treat in one's own home vs. going to a provider to get an injection. Patients do have to remember to take one more pill daily.
- Is consumption of sugar harmful to PCa? I presented this question because we had a discussion in a recent round table meeting and there appears to be ambiguity regarding this issue. Answer: The body breaks down all foods into glucose. Both noncancerous and cancerous cells feed on glucose. Dr. Fawole would not deprive body cells of glucose in an attempt to deprive cancer cells of glucose. Moderation is important. However, indirectly, too much glucose can lead to diabetes and blocked arteries. Because of diabetes, clogged arteries inhibits the flow of drugs to the cells where those drugs are needed.
- Does Relugolix act the same way as casodex? The two drugs employ different methods. One acts on the hormone producing agent and one acts on the receptor. Relugolix has a larger scale impact than Casodex.
- Can Relugolix be taken intermittently? No. In the study, Relugolix was taken daily.
- Is there a stage of life where genetic testing adds value? For instance, PSA tests are recommended for men over 45 years of age. At this point, guidelines do not recommend genetic testing unless cancer has been diagnosed. However, if a close relative has been diagnosed with cancer, depending upon the type of cancer, genetic testing may be appropriate.
- BRCA1&2: If one parent gets tested and is cleared of these gene mutations, that does not mean that the offspring is risk free from germline exposure. Both parents can pass on this gene mutation. Both parents should be tested. Dr. also mentioned that there are 16 homologous genes that are related to PCa. The key ones are the BRACA1&2, PALBN2 and CHEK
- When is it appropriate to combine hormone therapy with radiation therapy? If a patient has advanced PCa (outside the prostate) as opposed to localized, hormone therapy is normally recommended with radiation therapy. High risk patients based upon Gleason score, even though localized, should normally have hormone therapy along with radiation. The current standard is Lupron shots along with radiation.
- Can Relugolix be used with radiation instead of Lupron? Not at the present time. Dr. projects that some time in the future, this will be allowed. Based upon his experience with the FDA, he feels that the agency will require another clinical trial before it approves Relugolix with radiation.
- Define advanced prostate cancer. If the cancer is outside the prostate, it is considered advanced. If it is contained in the prostate, it is localized. Gleason scores define risk level. High gleason score cancers localized in the prostate are considered aggressive cancers. They have a high risk of spreading outside the prostate.
- Does your practice use a team approach? The simple answer is yes. The treating physician will sit with a team which may include pathologists, surgeons, radiologists and posit his recommendations and obtain opinions from the other members in the meeting.
- Rising PSA. One participant posed a question about a rising PSA. He was diagnosed 7 years ago, has a Gleason 6 and his PSA went from 3.1 to 6.4 in the seven years. Dr. would that consider that circumstance slow growing and expressed the concern focuses upon PSA doubling time. If PSA double in one year or less, that is usually an indication of growing cancer. The person also indicated that he is on Tamsulosin. Dr. Fawole indicated that this can have an adverse effect upon PSA results. One week prior to the test would be a reasonable time to temporarily stop taking Tamsulosin.
- Can prostatitis raise the PSA level? Yes it can, and the more severe the infection, the more drastic the effect.

|
Monthly Meeting January 6, 2021
Dr. Curtis Bryant, Assistant Professor in the Department of Radiation Oncology at the University of Florida. Dr. Bryant was our speaker for our virtual meeting on Wednesday, January 6, 2021. |
Our speaker for our virtual meeting on January 7, 2021, was Dr. Curtis Bryant of the UF Proton Therapy Institute in Jacksonville, FL. Dr. Bryant is an Assistant Professor in the Department of Radiation Oncology at the University of Florida. He specializes in the care of patients with prostate cancer, head and neck cancer and for patients with metastatic cancer. He received his undergraduate degree from Mary Washington University and medical degree from the University of North Carolina at Chapel Hill. He also received a Masters of Public Health from the University of North Carolina at Chapel Hill. He completed his residency training at the University of Florida. A burgeoning cancer researcher, he is the author of the recently published article Five-Year Biochemical Results, Toxicity, and Patient-Reported Quality of Life After Delivery of Dose-Escalated Image Guided Proton Therapy for Prostate Cancer which has documented the efficacy and safety of proton therapy for prostate cancer in a study that included over 1,300 patients treated at the University of Florida.
Since Dr. Burton does not know how much his audience knows about Prostate Cancer (PCa) his first several slides presented background information concerning PCa.
- SBRT is a method of delivering extremely high doses of radiation over a very short period of time and can be delivered by either Proton Therapy or IMRT.
- Brachytherapy can be either permanent where seeds are placed into the P and left there or temporary whereby high dose rods are placed into the P and taken out after 30 days.
Proton Therapy
Since Dr. Burton does not know how much his audience knows about Prostate Cancer (PCa) his first several slides presented background information concerning PCa.
- He presented slides showing the anatomy of the Prostate (P). He explained the anatomy and noted that the majority of the prostate is comprised of glands with some muscle tissue.
- Statistics: PCa is the #1 non skin cancer with 191,930 cases in 2020 and the #1 cancer killer with 33,330 deaths based upon info from the American Cancer Society.
- Risk Factors: Increased Age, African American Race, Dietary Fat, Genetic, Family Heritage
- Age risk: 40 - 59, 1 in 38; 60 - 69, 1 in 15; > 70, 1 in 8.
- Most men diagnosed are asymptomatic.
- Names for PCa are Prostate or Prostatic Adenocarcinomas, basically a cancer of glands. The primary purpose of glands is to secrete certain materials. When they no longer function properly, cancer can develop.
- 70% of PCa's are low risk; without treatment, cancer causing deaths without treatment is 1-2%
- 70% of cancers are in the back of the P, reason for Digital Rectal Exams.
- Biopsies should be performed for men over 75 when PSA is over 4 and abnormal DRE and for men 45 to 75 when PSA is 3 and abnormal DRE
- Gleason Score categorizes PCa into one of five grades. Dr.'s slide showed a grapic of what the different grades look like under a microscope.
- Before seeing him, Dr. prefers patients to know their PSA, Stage, Gleason, and Rsk Group
- Dr. presented a slide that specified the qualifications of Low, Intermediate and High risk groups
- Molecular studies also estimate risk groups: Prolaris, oncotypeDX, Decipher
- Treatment Option include 1) Active Surveillance,2) Prostatectomy, 3) Radiation 4)HIFU and 5) Cryotherapy
- SBRT is a method of delivering extremely high doses of radiation over a very short period of time and can be delivered by either Proton Therapy or IMRT.
- Brachytherapy can be either permanent where seeds are placed into the P and left there or temporary whereby high dose rods are placed into the P and taken out after 30 days.
Proton Therapy
- Type of external radiation that can be used to treat PCa and uses protons as opposed to X-rays (Photons.).
- Protons deposit most of their energy at the end of the beams path.
- A slide showed the difference of a proton beam vs a photon beam. The graphic presented a view of the subject lying on his stomach. The photon beam penetrated through the body while the proton beam stopped at the target. Under photon, the bowel and the kidneys are getting extra radiation.
- Decades were required to develop the technology to become clinically available, from the 1950's when universities initiated it till the 1990's when the first equipment was introduced at Loma Linda University in California.
- To be effective, the proton must approach the speed of light. Protons have a high degree of mass as compared to electrons.
- Proton machines use cyclotrons to generate protons and accelerate them to the speed of light and then deliver them via magnets to multiple gantries where patients are treated on a staggered basis.
- Dr. Burton then presented slides which presented the photos of the equipment. Massive. A picture of a gantry showed men working on it giving an idea of the size.
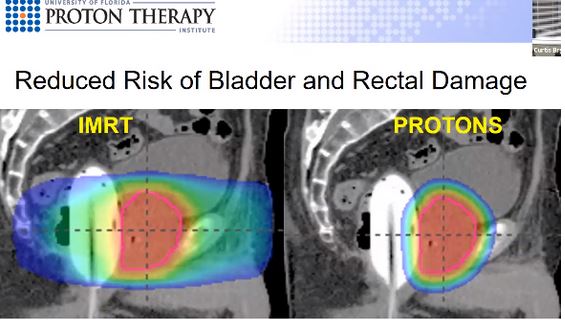
- A graphic showed a cross section of the pelvis with IMRT on one side and proton on the other. The IMRT side showed beams entering the body from eight different directions compared to two on the proton side, one beam on each hip. With proton, less dose to the rectum and to the bladder. Proton therapy eliminates more radiation that goes outside the P, but cannot get rid of all of it because of the anatomy of the P.
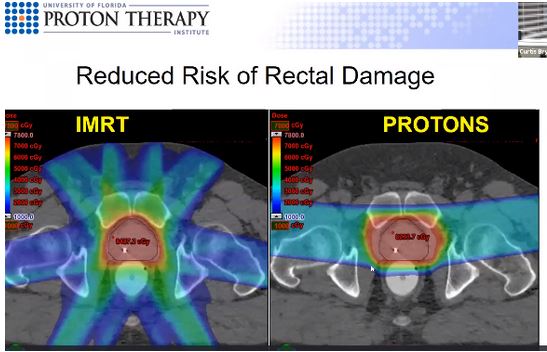
Dr. Bryant presented another graphic which compared IMRT to Proton Therapy. In this graphic, the front of the torso is on the right side of the graphic.
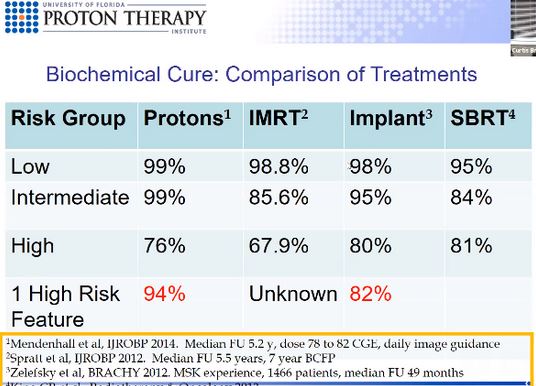
- Dr. Bryant et. al. performed a study of 1,327 men from 2006 through 2016 that were treated at his facility. Biochemical cure, which Dr. Bryant defined a situation where PSA does not rise after treatment, after 5 years for low risk disease was 99% with 94% for the intermediate group and 74% for the high risk group.
- Comparison to other forms of radiation treatment.
- Outcomes: With Proton Therapy, the urinary toxicity rate is 3% and the gastrointestinal toxicity rate is 0.6%, Compared to X-Ray radiation, there is a reduced risk of rectal urgency, second malignancies and reduced impact of testicular function.
- Erectile dysfunction: Risk is low if patient is able to perform satisfactorily before treatment.
- Risk of Side Effects: Major rectal bleeding <1%, 14.5% overall; Bladder or urethral bleeding, 3% overall.
- SpaceOar gel: The UF Proton Therapy Uses it as standard procedure. SpaceOar has reduced rectal problems from radiation by 70%. Dr. presented a graphic that showed an MRI image with and without SpaceOar. The gel provides a 1% cushion.
- PartiQol Study: This is a randomized study of 400 men put form by Massachusetts General Hospital, Harvard Center. The study compares quality of life (focusing upon bowel, urinary and erectile function) after 24 months, Proton Therapy to IMRT. The Study is looking at two different outcomes, the first outcome is mentioned in the prior sentence. Those outcomes will most likely be published in 2022 or 2023. The second outcome is cure rates, and that takes about five years.
- COMPARE Study: Forty two centers across the country are participating in this trail. This again compares IMRT to Proton Therapy. This includes comparison of the standard 39 treatments and the shorter 20 or 28 treatments. The goal is to have 3,000 patients, and they just reached 1,000. It will be several years before the study is published.
- PR-11 Study; This is for patients with high risk disease and the study is currently enrolling. In this study, the entire gland is treated with standard dosage but the areas of the tumor are treated with higher dosages.
- Proton Therapy is effective for low, intermediate and high risk disease.
- Overall cure rate is 94%
- SpaceOar gel reduces the risk of rectal bleeding.
- New protocols are available to compare proton therapy to X-ray and to improve tumor control for high risk cancer patients.
- How long does it take to get start treatment once the patient decides to embark upon Proton Therapy? Usually two weeks. If insurance declines payment, then the time can stretch to three or four weeks. The center has been quite successful in negotiating with insurance companies through peer to peer discussions with review doctors at the insurance companies. There are some insurance companies that absolutely refuse to reimburse protong therapy. In those situations, UF will inform the patient up front. Proton Therapy is covered by Medicare.
Fred Barone
[email protected]
Disclaimer: The Villages Prostate Group does not recommend or endorse the speakers, publications or descriptions of publications. They are simply provided as additional resources for your information.
